

Methods and indicators to validate country reductions in incidence of hepatitis C virus infection to elimination levels set by WHO
- PMID: 35122713
- PMCID: PMC10644895
- DOI: 10.1016/S2468-1253(21)00311-3
Methods and indicators to validate country reductions in incidence of hepatitis C virus infection to elimination levels set by WHO
Abstract
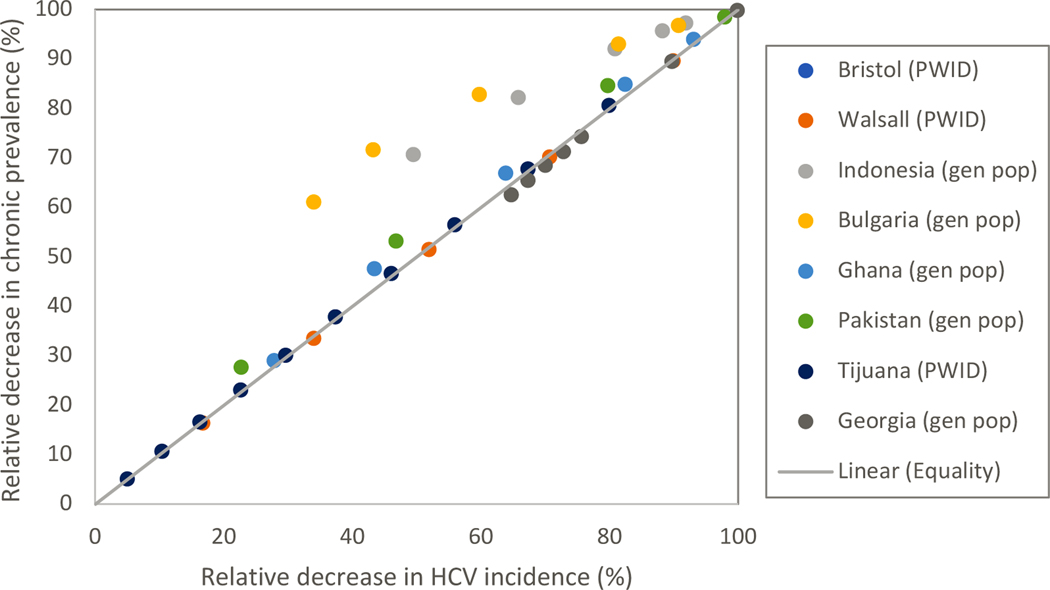
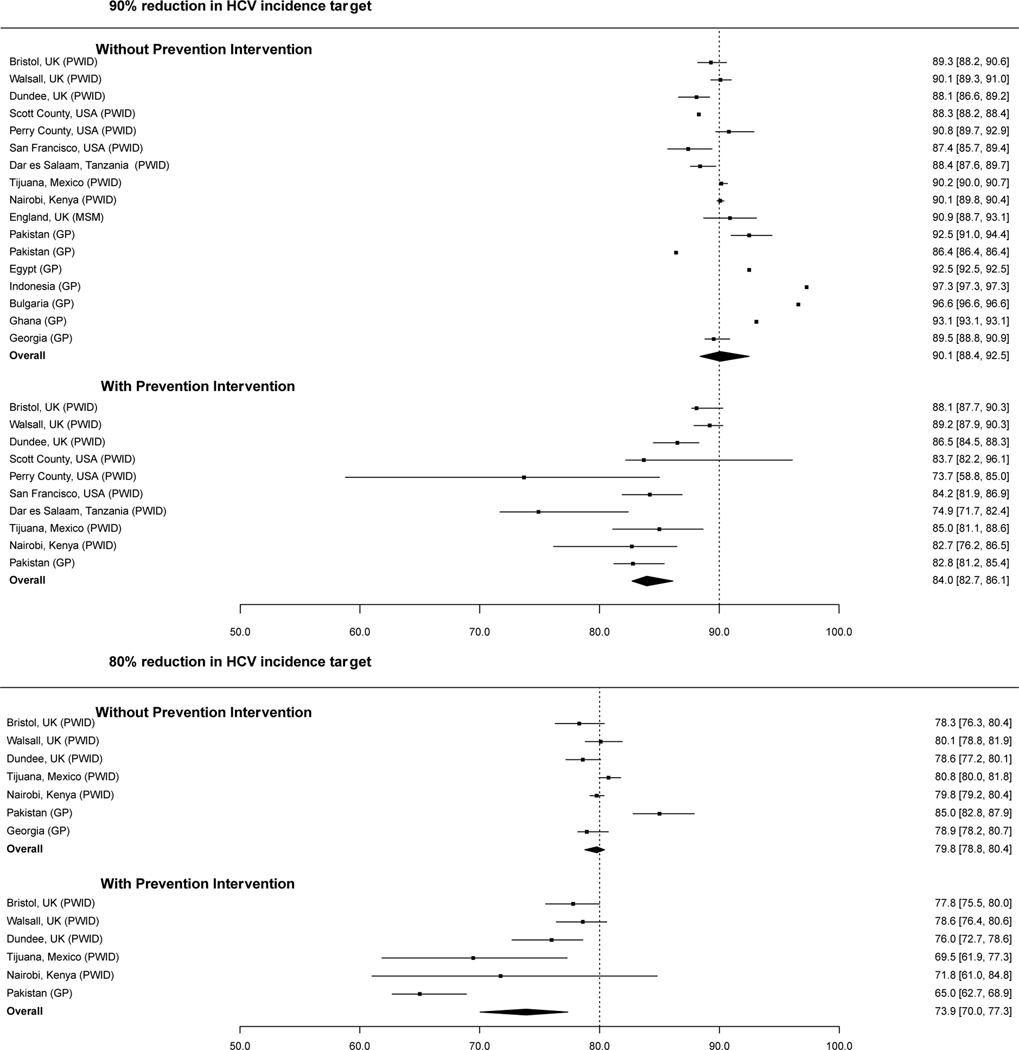
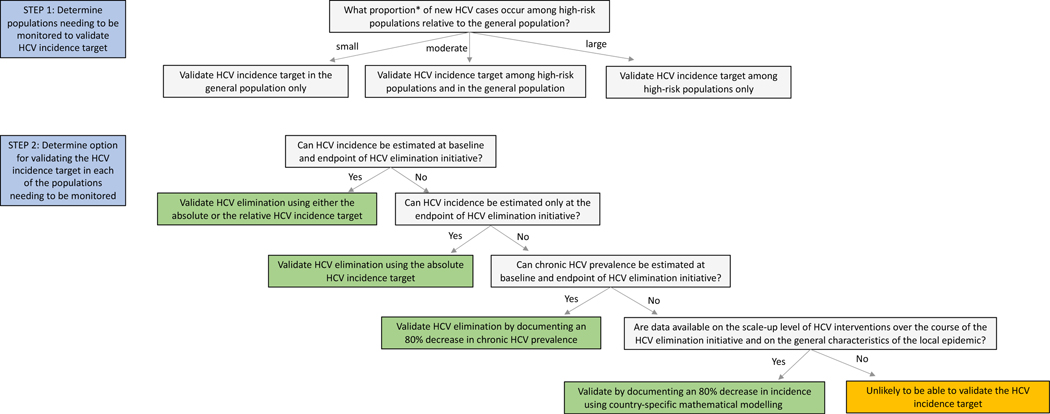
One of the main goals of the 2016 Global Health Sector Strategy on viral hepatitis is the elimination of hepatitis C virus (HCV) as a public health problem by 2030, defined as an 80% reduction in incidence and 65% reduction in mortality relative to 2015. Although monitoring HCV incidence is key to validating HCV elimination, use of the gold-standard method, which involves prospective HCV retesting of people at risk, can be prohibitively resource-intensive. Additionally, few countries collected quality data in 2015 to enable an 80% decrease by 2030 to be calculated. Here, we first review different methods of monitoring HCV incidence and discuss their resource implications and applicability to various populations. Second, using mathematical models developed for various global settings, we assess whether trends in HCV chronic prevalence or HCV antibody prevalence or scale-up levels for HCV testing, treatment, and preventative interventions can be used as reliable alternative indicators to validate the HCV incidence target. Third, we discuss the advantages and disadvantages of an absolute HCV incidence target and suggest a suitable threshold. Finally, we propose three options that countries can use to validate the HCV incidence target, depending on the available surveillance infrastructure.
Copyright © 2022 World Health Organization. Published by Elsevier Ltd. All rights reserved. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests PV and JGW have received unrestricted research grants from Gilead, outside the submitted work. JGW has also recieved a research grant from FIND outside the submitted work. NM has received unrestricted research grants from Gilead and Merk outside the submitted work. MH has received speaker fees honoraria in past 5 years from Gilead and Merck Shape & Dohme (MSD). HF has received an honorarium from MSD unrelated to this research. HF, ZW, and PV declare payment to their institution from WHO to prepare a background paper that formed the basis for this paper. All other authors declare no competing interests.
Figures
References
-
- World Health Organization. Global health sector strategy on viral hepatitis 2016–2021. Geneva, Switzerland: World Health Organization, 2016. Available at: http://apps.who.int/iris/bitstream/10665/246177/1/WHO-HIV-2016.06eng.pdf.... Accessed August 2017.
-
- Martin NK, Hickman M, Hutchinson SJ, Goldberg DJ, Vickerman P. Combination interventions to prevent HCV transmission among people who inject drugs: modeling the impact of antiviral treatment, needle and syringe programs, and opiate substitution therapy. Clin Infect Dis 2013; 57 Suppl 2: S39–45. - PMC - PubMed
-
- World Health Organization. Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Geneva, Switzerland: World Health Organization, 2021. Available at: https://www.who.int/publications/i/item/9789240027077. Accessed June 2021.
-
- Shiha G, Soliman R, Mikhail NNH, Easterbrook P. Reduced incidence of hepatitis C in 9 villages in rural Egypt: Progress towards national elimination goals. J Hepatol 2021; 74(2): 303–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
