

AGA Clinical Practice Update on the Personalized Approach to the Evaluation and Management of GERD: Expert Review
- PMID: 35123084
- PMCID: PMC9838103
- DOI: 10.1016/j.cgh.2022.01.025
AGA Clinical Practice Update on the Personalized Approach to the Evaluation and Management of GERD: Expert Review
Erratum in
-
Correction.Clin Gastroenterol Hepatol. 2022 Sep;20(9):2156. doi: 10.1016/j.cgh.2022.05.005. Epub 2022 Jul 9. Clin Gastroenterol Hepatol. 2022. PMID: 35820983 No abstract available.
Abstract
Background & aims: As many as one-half of all patients with suspected gastroesophageal reflux disease (GERD) do not derive benefit from acid suppression. This review outlines a personalized diagnostic and therapeutic approach to GERD symptoms.
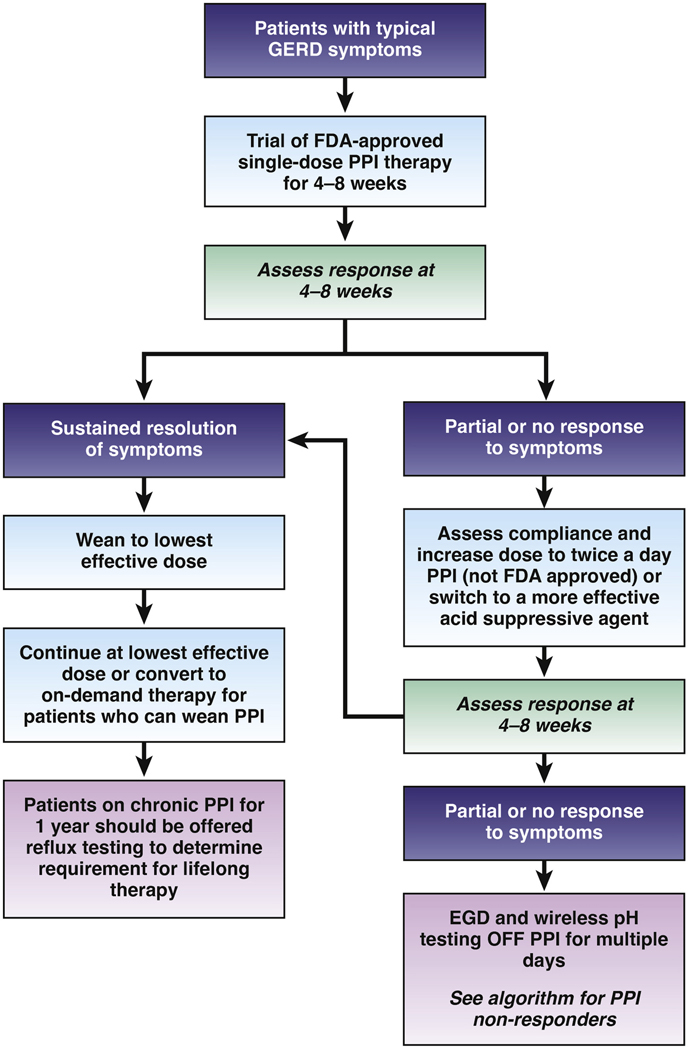
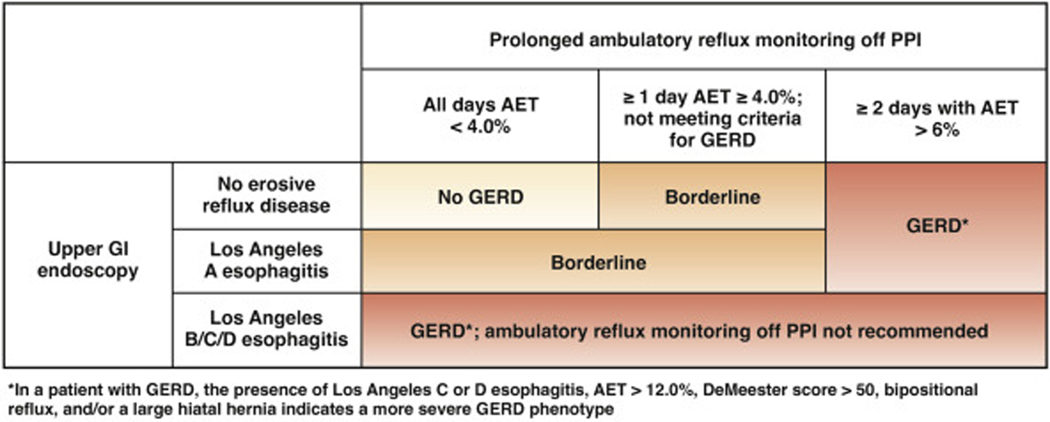
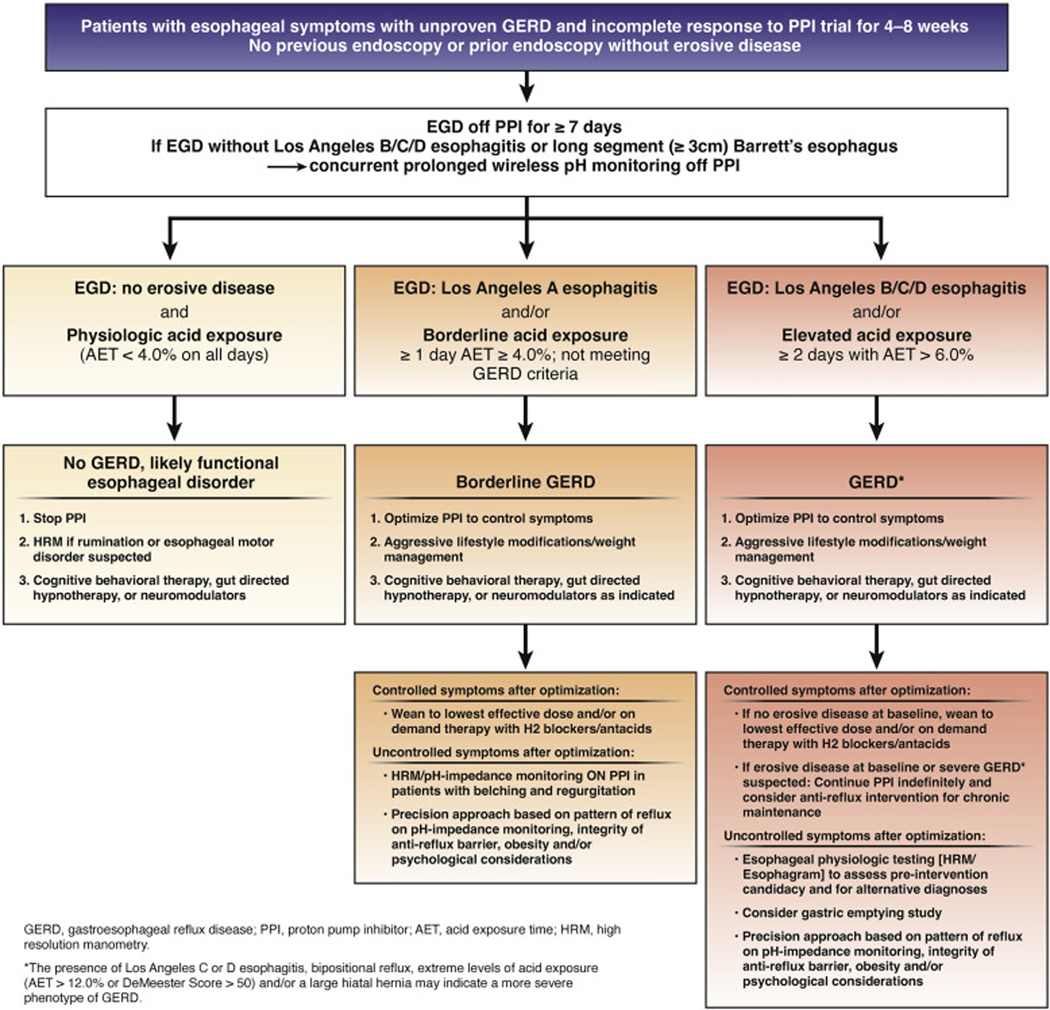
Methods: The Best Practice Advice statements presented here were developed from expert review of existing literature combined with extensive discussion and expert opinion to provide practical advice. Formal rating of the quality of evidence or strength of recommendations was not the intent of this clinical practice update. BEST PRACTICE ADVICE 1: Clinicians should develop a care plan for investigation of symptoms suggestive of GERD, selection of therapy (with explanation of potential risks and benefits), and long-term management, including possible de-escalation, in a shared-decision making model with the patient. BEST PRACTICE ADVICE 2: Clinicians should provide standardized educational material on GERD mechanisms, weight management, lifestyle and dietary behaviors, relaxation strategies, and awareness about the brain-gut axis relationship to patients with reflux symptoms. BEST PRACTICE ADVICE 3: Clinicians should emphasize safety of proton pump inhibitors (PPIs) for the treatment of GERD. BEST PRACTICE ADVICE 4: Clinicians should provide patients presenting with troublesome heartburn, regurgitation, and/or non-cardiac chest pain without alarm symptoms a 4- to 8-week trial of single-dose PPI therapy. With inadequate response, dosing can be increased to twice a day or switched to a more effective acid suppressive agent once a day. When there is adequate response, PPI should be tapered to the lowest effective dose. BEST PRACTICE ADVICE 5: If PPI therapy is continued in a patient with unproven GERD, clinicians should evaluate the appropriateness and dosing within 12 months after initiation, and offer endoscopy with prolonged wireless reflux monitoring off PPI therapy to establish appropriateness of long-term PPI therapy. BEST PRACTICE ADVICE 6: If troublesome heartburn, regurgitation, and/or non-cardiac chest pain do not respond adequately to a PPI trial or when alarm symptoms exist, clinicians should investigate with endoscopy and, in the absence of erosive reflux disease (Los Angeles B or greater) or long-segment (≥3 cm) Barrett's esophagus, perform prolonged wireless pH monitoring off medication (96-hour preferred if available) to confirm and phenotype GERD or to rule out GERD. BEST PRACTICE ADVICE 7: Complete endoscopic evaluation of GERD symptoms includes inspection for erosive esophagitis (graded according to the Los Angeles classification when present), diaphragmatic hiatus (Hill grade of flap valve), axial hiatus hernia length, and inspection for Barrett's esophagus (graded according to the Prague classification and biopsied when present). BEST PRACTICE ADVICE 8: Clinicians should perform upfront objective reflux testing off medication (rather than an empiric PPI trial) in patients with isolated extra-esophageal symptoms and suspicion for reflux etiology. BEST PRACTICE ADVICE 9: In symptomatic patients with proven GERD, clinicians should consider ambulatory 24-hour pH-impedance monitoring on PPI as an option to determine the mechanism of persisting esophageal symptoms despite therapy (if adequate expertise exists for interpretation). BEST PRACTICE ADVICE 10: Clinicians should personalize adjunctive pharmacotherapy to the GERD phenotype, in contrast to empiric use of these agents. Adjunctive agents include alginate antacids for breakthrough symptoms, nighttime H2 receptor antagonists for nocturnal symptoms, baclofen for regurgitation or belch predominant symptoms, and prokinetics for coexistent gastroparesis. BEST PRACTICE ADVICE 11: Clinicians should provide pharmacologic neuromodulation, and/or referral to a behavioral therapist for hypnotherapy, cognitive behavioral therapy, diaphragmatic breathing, and relaxation strategies in patients with functional heartburn or reflux disease associated with esophageal hypervigilance reflux hypersensitivity and/or behavioral disorders. BEST PRACTICE ADVICE 12: In patients with proven GERD, laparoscopic fundoplication and magnetic sphincter augmentation are effective surgical options, and transoral incisionless fundoplication is an effective endoscopic option in carefully selected patients. BEST PRACTICE ADVICE 13: In patients with proven GERD, Roux-en-Y gastric bypass is an effective primary anti-reflux intervention in obese patients, and a salvage option in non-obese patients, whereas sleeve gastrectomy has potential to worsen GERD. BEST PRACTICE ADVICE 14: Candidacy for invasive anti-reflux procedures includes confirmatory evidence of pathologic GERD, exclusion of achalasia, and assessment of esophageal peristaltic function.
Keywords: Ambulatory Reflux Monitoring; Gastroesophageal Reflux Disease; Proton Pump Inhibitors.
Copyright © 2022 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 2006; 101:1900–1920, quiz: 1943. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
