

The gut hormone glucose-dependent insulinotropic polypeptide is downregulated in response to myocardial injury
- PMID: 35123462
- PMCID: PMC8817614
- DOI: 10.1186/s12933-022-01454-3
The gut hormone glucose-dependent insulinotropic polypeptide is downregulated in response to myocardial injury
Abstract
Background: The gut incretin hormones GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic peptide) are secreted by enteroendocrine cells following food intake leading to insulin secretion and glucose lowering. Beyond its metabolic function GIP has been found to exhibit direct cardio- and atheroprotective effects in mice and to be associated with cardiovascular prognosis in patients with myocardial infarction. The aim of this study was to characterize endogenous GIP levels in patients with acute myocardial infarction.
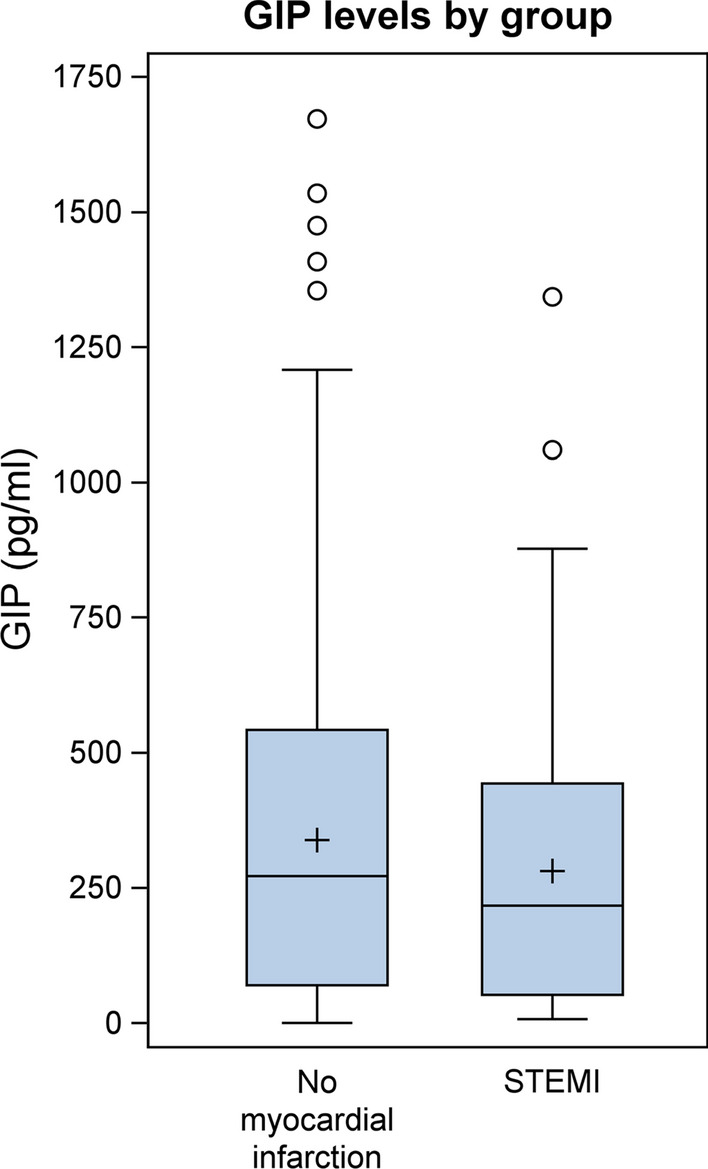
Methods and results: Serum concentrations of GIP were assessed in 731 patients who presented with clinical indication of coronary angiography. Circulating GIP levels were significantly lower in patients with STEMI (ST-elevation myocardial infarction; n=100) compared to clinically stable patients without myocardial infarction (n=631) (216.82 pg/mL [Q1-Q3: 52.37-443.07] vs. 271.54 pg/mL [Q1-Q3: 70.12-542.41], p = 0.0266). To characterize endogenous GIP levels in patients with acute myocardial injury we enrolled 18 patients scheduled for cardiac surgery with cardiopulmonary bypass and requirement of extracorporeal circulation as a reproducible condition of myocardial injury. Blood samples were drawn directly before surgery (baseline), upon arrival at the intensive care unit (ICU), 6 h post arrival to the ICU and at the morning of the first and second postoperative days. Mean circulating GIP concentrations decreased in response to surgery from 45.3 ± 22.6 pg/mL at baseline to a minimum of 31.9 ± 19.8 pg/mL at the first postoperative day (p = 0.0384) and rose again at the second postoperative day (52.1 ± 28.0 pg/mL).
Conclusions: Circulating GIP levels are downregulated in patients with myocardial infarction and following cardiac surgery. These results might suggest nutrition-independent regulation of GIP secretion following myocardial injury in humans.
Keywords: Cardiac injury; Cardiac surgery; GIP; Incretin; Myocardial infarction.
© 2022. The Author(s).
Conflict of interest statement
The authors do not have any competing interest.
Figures

References
-
- Asmar M, Asmar A, Simonsen L, Gasbjerg LS, Sparre-Ulrich AH, Rosenkilde MM, Hartmann B, Dela F, Holst JJ, Bulow J. The gluco- and liporegulatory and vasodilatory effects of glucose-dependent insulinotropic polypeptide (GIP) are abolished by an antagonist of the human GIP receptor. Diabetes. 2017;66(9):2363–2371. doi: 10.2337/db17-0480. - DOI - PubMed
-
- Burgmaier M, Liberman A, Mollmann J, Kahles F, Reith S, Lebherz C, Marx N, Lehrke M. Glucagon-like peptide-1 (GLP-1) and its split products GLP-1(9-37) and GLP-1(28-37) stabilize atherosclerotic lesions in apoe(-)/(-) mice. Atherosclerosis. 2013;231(2):427–435. doi: 10.1016/j.atherosclerosis.2013.08.033. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
