

Metabolic imaging with FDG-PET and time to progression in patients discontinuing immune-checkpoint inhibition for metastatic melanoma
- PMID: 35123578
- PMCID: PMC8817553
- DOI: 10.1186/s40644-022-00449-3
Metabolic imaging with FDG-PET and time to progression in patients discontinuing immune-checkpoint inhibition for metastatic melanoma
Abstract
Background: The optimal duration of immune checkpoint blockade (ICB) therapy is not well established. Active residual disease is considered prohibitive for treatment discontinuation and its detection by diagnostic CT imaging is limited. Here, we set out to determine the potential added value of 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) to identify patients at higher risk of relapse following discontinuation of ICB in advanced melanoma.
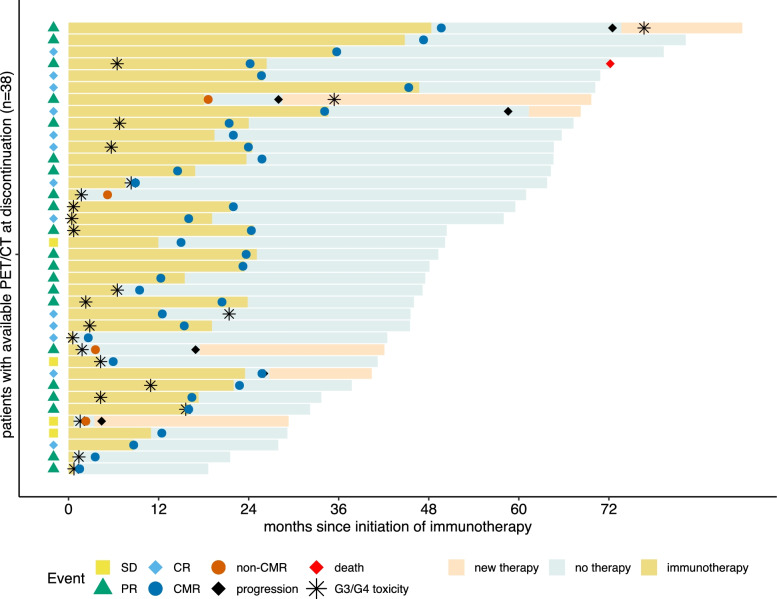
Methods: Metastatic melanoma patients who discontinued ICB were identified retrospectively. Eligible patients received FDG-PET and diagnostic CT within four months of ICB discontinuation. We defined morphologic response using RECIST v1.1. Complete metabolic response (CMR) was defined as uptake in tumor lesions below background, whereas any site of residual, FDG-avid disease was rated as non-CMR. The primary endpoint was time to progression (TTP) after therapy discontinuation stratified by morphologic and metabolic imaging response using Kaplan-Meier estimates and log-rank test.
Results: Thiry-eight patients were eligible for this analysis. Median follow-up was 37.3 months since ICB discontinuation. Median TTP in the overall cohort was not reached. A greater proportion of patients were rated as CMR in PET (n = 34, 89.5%) as compared to complete response (CR) in CT (n = 13, 34.2%). Median TTP was reached in patients with non-CMR (12.7 months, 95%CI 4.4-not reached) but not for patients with CMR (log-rank: p < 0.001). All patients with complete response by CT had CMR by PET. In a subset of patients excluding those with complete response by CT, TTP remained significantly different between CMR and non-CMR (log-rank: p < 0.001).
Conclusion: Additional FDG-PET at time of discontinuation of ICB therapy helps identify melanoma patients with a low risk of recurrence and favourable prognosis compared to CT imaging alone. Results may have clinical relevance especially for patients with residual tumor burden.
Keywords: Checkpoint inhibition; Discontinuation; FDG; Immunotherapy; Melanoma; PET.
© 2022. The Author(s).
Conflict of interest statement
JF has received fees from Eisai, outside of the submitted work. AZ received travel support from Novartis, Sanofi Genzyme, and Bristol-Myers Squibb, outside the submitted work. LZ received honoraria from Roche, BMS, MSD, Novartis, Pierre Fabre; Consultant or Advisory Role: BMS, Novartis, Pierre Fabre, Sunpharma, Sanofi, MSD; Research funding to institution: Novartis; Travel support: BMS, Pierre Fabre, Sanofi, Amgen, Novartis, Sunpharma. LU reports Speaker for Bayer Healthcare; Speaker and Research Grant Siemens Healtcare outside of the submitted work. VG reports grants, personal fees and non-financial support from Astra Zeneca, Bristol-Myers Squibb, MSD Sharp & Dohme, Ipsen, Pfizer. Personal fees from Merck Serono, EUSAPharm, Novartis, Eisai, Bayer, Roche, Janssen-Cilag, Lilly and PharmaMar. SU declares research support from Bristol Myers Squibb and Merck Serono; speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Merck Serono, Novartis and Roche, and travel support from Bristol Myers Squibb, and Merck Sharp & Dohme. EC received travel support from Bristol-Myers Squibb, Merck Sharp & Dohme, and Novartis, outside the submitted work. DS reports personal fees and non-financial support from Roche/Genentech, grants, personal fees, non-financial support and other from BMS, personal fees from Merck Sharp & Dohme, personal fees and non-financial support from Merck Serono, grant, personal fees and non-financial support from Amgen, personal fees from Immunocore, personal fees from Incyte, personal fees from 4SC, personal fees from Pierre Fabre, personal fees and non-financial support from Sanofi/Regeneron, personal fees from Array BioPharma, personal fees from Pfizer, personal fees from Philogen, personal fees from Regeneron, personal fees from Nektar, personal fees from Sandoz, grants, personal fees and non-financial support from Novartis, personal fees and non-financial support from SunPharma, Replimune, Helsinn, OncoSec and InFlaRx outside the submitted work. WPF is a consultant for BTG, and he received fees from RadioMedix, Bayer, and Parexel outside of the submitted work. EL served as consultant and/or has received honoraria from Amgen, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Medac, Sanofi, Sunpharma and travel support from Amgen, Merck Sharp & Dohme, Bristol-Myers Squibb, Pierre Fabre, Sunpharma and Novartis, outside the submitted work. All others have nothing to disclose.
Figures

References
-
- Hodi FS, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Cowey CL, et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018;19(11):1480–1492. doi: 10.1016/S1470-2045(18)30700-9. - DOI - PubMed
-
- Robert C, Ribas A, Schachter J, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019;20(9):1239–1251. doi: 10.1016/S1470-2045(19)30388-2. - DOI - PubMed
-
- Ascierto PA, Long GV, Robert C, Brady B, Dutriaux C, Di Giacomo AM, et al. Survival outcomes in patients with previously untreated BRAF wild-type advanced melanoma treated with nivolumab therapy: three-year follow-up of a randomized phase 3 trial. JAMA Oncol. 2019;5(2):187–194. doi: 10.1001/jamaoncol.2018.4514. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
