

Trametinib versus standard of care in patients with recurrent low-grade serous ovarian cancer (GOG 281/LOGS): an international, randomised, open-label, multicentre, phase 2/3 trial
- PMID: 35123694
- PMCID: PMC8819271
- DOI: 10.1016/S0140-6736(21)02175-9
Trametinib versus standard of care in patients with recurrent low-grade serous ovarian cancer (GOG 281/LOGS): an international, randomised, open-label, multicentre, phase 2/3 trial
Abstract
Background: Low-grade serous carcinoma of the ovary or peritoneum is characterised by MAPK pathway aberrations and its reduced sensitivity to chemotherapy relative to high-grade serous carcinoma. We compared the MEK inhibitor trametinib to physician's choice standard of care in patients with recurrent low-grade serous carcinoma.
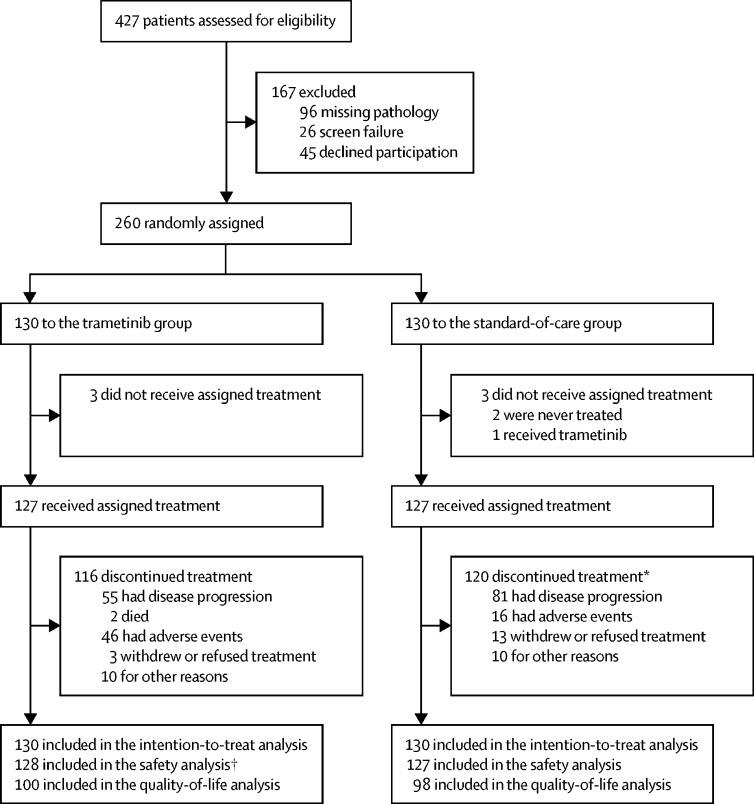
Methods: This international, randomised, open-label, multicentre, phase 2/3 trial was done at 84 hospitals in the USA and UK. Eligible patients were aged 18 years or older with recurrent low-grade serous carcinoma and measurable disease, as defined by Response Evaluation Criteria In Solid Tumors version 1.1, had received at least one platinum-based regimen, but not all five standard-of-care drugs, and had received an unlimited number of previous regimens. Patients with serous borderline tumours or tumours containing low-grade serous and high-grade serous carcinoma were excluded. Eligible patients were randomly assigned (1:1) to receive either oral trametinib 2 mg once daily (trametinib group) or one of five standard-of-care treatment options (standard-of-care group): intravenous paclitaxel 80 mg/m2 by body surface area on days 1, 8, and 15 of every 28-day cycle; intravenous pegylated liposomal doxorubicin 40-50 mg/m2 by body surface area once every 4 weeks; intravenous topotecan 4 mg/m2 by body surface area on days 1, 8, and 15 of every 28-day cycle; oral letrozole 2·5 mg once daily; or oral tamoxifen 20 mg twice daily. Randomisation was stratified by geographical region (USA or UK), number of previous regimens (1, 2, or ≥3), performance status (0 or 1), and planned standard-of-care regimen. The primary endpoint was investigator-assessed progression-free survival while receiving randomised therapy, as assessed by imaging at baseline, once every 8 weeks for 15 months, and then once every 3 months thereafter, in the intention-to-treat population. Safety was assessed in patients who received at least one dose of study therapy. This trial is registered with ClinicalTrials.gov, NCT02101788, and is active but not recruiting.
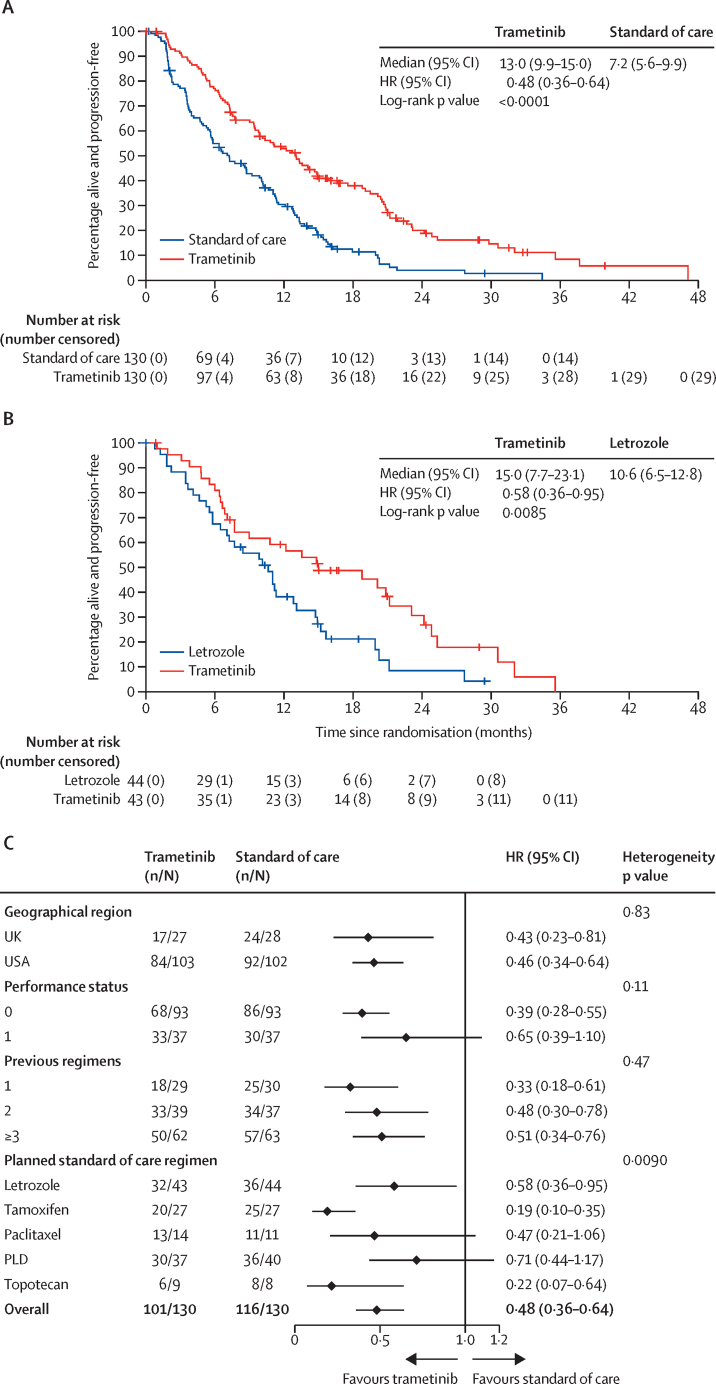
Findings: Between Feb 27, 2014, and April 10, 2018, 260 patients were enrolled and randomly assigned to the trametinib group (n=130) or the standard-of-care group (n=130). At the primary analysis, there were 217 progression-free survival events (101 [78%] in the trametinib group and 116 [89%] in the standard-of-care group). Median progression-free survival in the trametinib group was 13·0 months (95% CI 9·9-15·0) compared with 7·2 months (5·6-9·9) in the standard-of-care group (hazard ratio 0·48 [95% CI 0·36-0·64]; p<0·0001). The most frequent grade 3 or 4 adverse events in the trametinib group were skin rash (17 [13%] of 128), anaemia (16 [13%]), hypertension (15 [12%]), diarrhoea (13 [10%]), nausea (12 [9%]), and fatigue (ten [8%]). The most frequent grade 3 or 4 adverse events in the standard-of-care group were abdominal pain (22 [17%]), nausea (14 [11%]), anaemia (12 [10%]), and vomiting (ten [8%]). There were no treatment-related deaths.
Interpretation: Trametinib represents a new standard-of-care option for patients with recurrent low-grade serous carcinoma.
Funding: NRG Oncology, Cancer Research UK, Target Ovarian Cancer, and Novartis.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests DMG reports payments made to his institution from the National Cancer Institute (NRG Oncology), Novartis, and the GOG Foundation for this study; royalties or licenses from Elsevier and UpToDate outside the submitted work; consulting fees from Genentech outside the submitted work; personal fees for service as a member of the Committee of the National Cancer Institute outside the submitted work; and stock or stock options from Johnson & Johnson, Bristol Myers Squibb, and Biogen outside the submitted work. AM reports service as a masked study statistician for VBL Therapeutics; provision of statistical institutional support for Advaxis; service as a data safety monitoring board reporting statistician for Regeneron; and service on a study steering committee for Genentech and AstraZeneca, all outside the submitted work. RLC reports consulting fees from AstraZeneca, Merck–GlaxoSmithKline, and Clovis; grants from Genmab, Genentech–Roche, Janssen, Agenus, Regeneron, and OncoQuest; payments or honoraria for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from AstraZeneca, Merck–GlaxoSmithKline, and Clovis; and service on a data safety monitoring board or an advisory board for Janssen, VBL Therapeutics, and AstraZeneca, all outside the submitted work. KNM reports service on advisory boards for Alkemeres, AstraZeneca, Aravive, Blueprint Medicines, Eisai, Elevar, GlaxoSmithKline–Tesaro, Genentech–Roche, Hengrui, Immunogen, IMab, Merck, Mereo, Mersana, Myriad, OncXerna, Onconova, Novartis, Sorrento, Tarveda, and VBL Therapeutics, all outside the submitted work; grant funding from PTC Therapeutics, Lilly, Merck, and Genentech–Roche outside the submitted work; funding paid to her institution from Cyteir, Immunocore, Bolt Bio, Amgen, Artios, GlaxoSmithKline–Tesaro, Mereo, Regeneron, Aravive, Verastem, and AstraZeneca, for all of which she also serves as a local principal investigator; serving as national principal investigator for the IMaGYN050 trial of ovarian cancer (Genentech–Roche), the MIRASOL trial of ovarian cancer (Immunogen), the Relevare study of ovarian cancer (OncXerna), the FIRST study of ovarian cancer (GlaxoSmithKline–Tesaro), and the ETCTN 10422 study of ovarian cancer (National Cancer Institute); being the associate director for GOG Partners, on the GOG Foundation board of directors, and the NRG Oncology chair of the ovarian cancer committee; and receiving speaking reimbursement from PER, Research to Practice, Medscape, Great Debates and Updates, and Gyn Mal, all of which are outside the scope of this work but were active during the conduct of this study. SB reports grants paid to their institution from AstraZeneca, Tesaro, and GlaxoSmithKline; personal fees for participation in advisory boards from Amgen, AstraZeneca, Genmab, GlaxoSmithKline, Immunogen, Merck Sharp & Dohme, Merck Serono, Mersana, Oncxerna, Seagen, Shattuck Lab, and Epsilogen; and personal fees for lectures from Amgen, AstraZeneca, Clovis, GlaxoSmithKline, Immunogen, Merck Sharp & Dohme, Mersana, Pfizer, Roche, and Takeda, all outside the submitted work. AAS reports a National Cancer Trial Network grant; grants paid to her institution from AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Clovis, Eisai, Immutep, Merck, OncoQuest, PharmaMar, Genentech–Roche, Seagen, Tesaro–GlaxoSmithKline, and VBL Therapeutics; consulting fees from Aravive, AstraZeneca, Clovis, Cordgenics, Eisai, Merck, Mersana, Myriad, Oncoquest, Genentech–Roche, and Tesaro–GlaxoSmithKline; presentations for educational events on cervical cancer sponsored by Research to Practice; service on advisory boards (uncompensated) for AbbVie and Regeneron; service on clinical trial steering committees (all uncompensated) for the AtTEnd trial (Hoffman-LaRoche), the Oval Trial (VBL Therapeutics), and the FLORA-5 trial (Oncoquest); and service on the GOG Foundation Board of Directors, the Society of Gynecologic Oncology Board of Directors, and the American Association of Obstetricians and Gynecologists Foundation Board of Trustees, all outside the submitted work. DMO reports National Cancer Institute support for this clinical trial; research funding paid to their institution from AstraZeneca, Tesaro–GlaxoSmithKline, Immunogen, Janssen–Johnson & Johnson, AbbVie Regeneron, Amgen, Novocure, Genentech–Roche, VentiRx Array Biopharma EMD Serono, Ergomed, Ajinomoto, Ludwig Cancer Research Stemcentrx, Cerulean Pharma, the GOG Foundation, the National Cancer Institute, Bristol Myers Squibb, C Serono, TRACON Pharmaceuticals, Yale University, New Mexico Cancer Care Alliance, inVentiv Health Clinical, Iovance Biotherapeutics, PRA Intl, Eisai, Agenus, Merck, GenMab, SeaGen, Mersana, and Clovis; personal fees for consulting or advisory board membership, or both, from AstraZeneca, Tesaro–GlaxoSmithKline, Immunogen, Ambry, Janssen–Johnson & Johnson, BBI, Agenus, AbbVie, Regeneron, Amgen, Novocure, Genentech–Roche, GOG Foundation, Iovance Biotherapeutics, Myriad Genetics, Eisai, Agenus, Tarveda, Merck, SeaGen, Novartis, Mersana, Clovis, Rubius, and Elevar, all outside the submitted work. OD reports grants or contracts from AstraZeneca, Clovis, Genentech, AbbVie, IMV, Millenium, and Pharmamar; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Tesaro–GlaxoSmithKline and AstraZeneca; payment for expert testimony in one legal case unrelated to the current study; and participation on a data safety monitoring board or advisory board for Merck, Clovis, PACT, and Genentech, all outside the submitted work. SG reports financial support paid to her institution for the present study from the National Clinical Trials Network; grants or contracts from AstraZeneca, AbbVie, Pfizer, Rigel, Iovance, Tesaro, Genentech–Roche, PharmaMar, and GlaxoSmithKline; patents licensed to Sermonix (US patent numbers 10,905,659 and 10,258,604); participation on a data safety monitoring board or advisory board for Sermonix, Elevar Therapeutics, and GlaxoSmithKline; and service as an NRG Oncology phase 1 subcommittee co-chair, all outside the submitted work. BS reports personal fees for service on advisory boards for Abbvie, AstraZeneca, Bostongene, Clovis, Eisai, Genentech, GlaxoSmithKline, Jazz Pharmaceticals, Lilly, Merck, Myriad, Novartis, Nuvation, Onconova, and Seagen; and consulting for the GOG Foundation, all outside the submitted work. AE reports grants or contracts from UKRI for a post-doctoral fellowship outside the submitted work. CG reports grants from GlaxoSmithKline and Novartis for this study (trametinib, the test drug, was sold by GlaxoSmithKline to Novartis during the course of the study). WEB, JP, KCa, WR, DM, KCo, HG, PH, JF, MC, RLH, CSH, HQH, and LW declare no competing interests.
Figures
Comment in
-
Targeting MAPK in recurrent, low-grade serous ovarian cancer.Lancet. 2022 Feb 5;399(10324):499-501. doi: 10.1016/S0140-6736(21)02338-2. Lancet. 2022. PMID: 35123677 No abstract available.
References
-
- Kurman RJ, Carcangiu ML, Herrington CS, Young RH. 4th edition. volume 6. International Agency For Research On Cancer; Lyon: 2014. WHO classification of tumours of the female reproductive organs: WHO classification of tumours.
-
- Prat J, D'Angelo E, Espinosa I. Ovarian carcinomas: at least five different diseases with distinct histological features and molecular genetics. Hum Pathol. 2018;80:11–27. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
