

Receiver operating characteristic curve: overview and practical use for clinicians
- PMID: 35124947
- PMCID: PMC8831439
- DOI: 10.4097/kja.21209
Receiver operating characteristic curve: overview and practical use for clinicians
Abstract
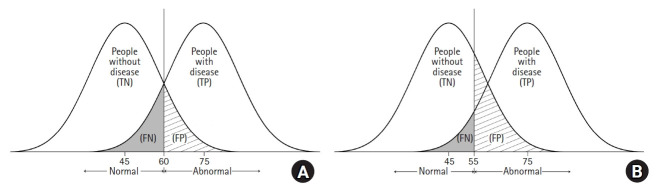
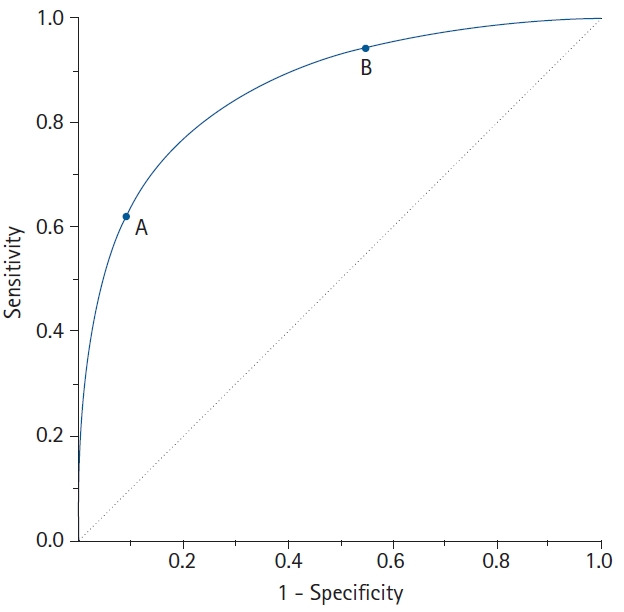
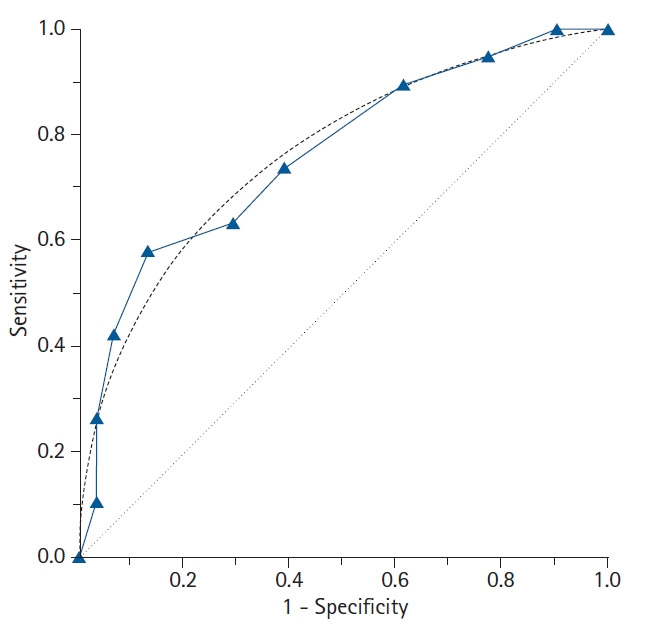
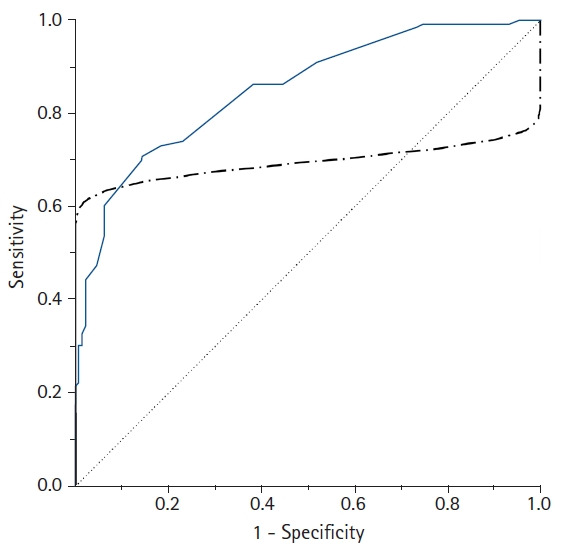
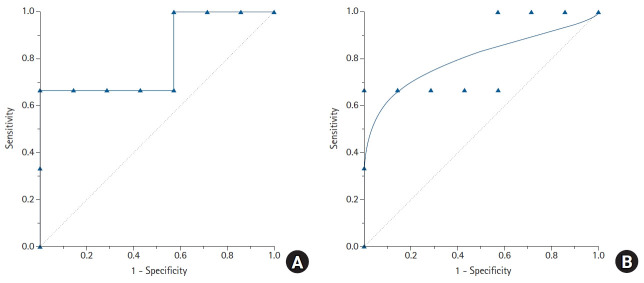
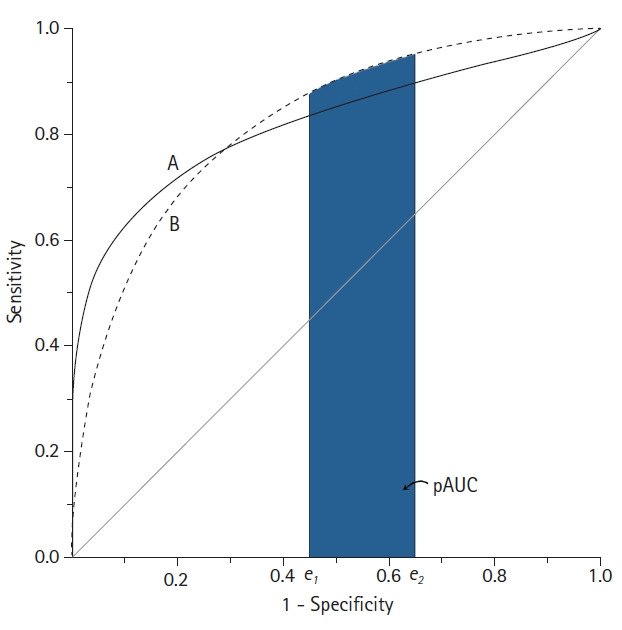
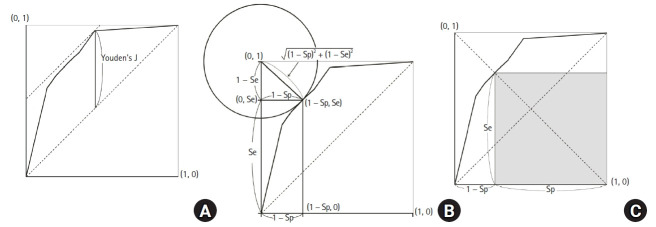
Using diagnostic testing to determine the presence or absence of a disease is essential in clinical practice. In many cases, test results are obtained as continuous values and require a process of conversion and interpretation and into a dichotomous form to determine the presence of a disease. The primary method used for this process is the receiver operating characteristic (ROC) curve. The ROC curve is used to assess the overall diagnostic performance of a test and to compare the performance of two or more diagnostic tests. It is also used to select an optimal cut-off value for determining the presence or absence of a disease. Although clinicians who do not have expertise in statistics do not need to understand both the complex mathematical equation and the analytic process of ROC curves, understanding the core concepts of the ROC curve analysis is a prerequisite for the proper use and interpretation of the ROC curve. This review describes the basic concepts for the correct use and interpretation of the ROC curve, including parametric/nonparametric ROC curves, the meaning of the area under the ROC curve (AUC), the partial AUC, methods for selecting the best cut-off value, and the statistical software to use for ROC curve analyses.
Keywords: Area under curve; Mathematics; ROC curve; Reference values; Research design; Routine diagnostic tests; Statistics.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
