

Evolution of a Paradigm Switch in Diagnosis and Treatment of HPV-Driven Head and Neck Cancer-Striking the Balance Between Toxicity and Cure
- PMID: 35126105
- PMCID: PMC8810823
- DOI: 10.3389/fphar.2021.753387
Evolution of a Paradigm Switch in Diagnosis and Treatment of HPV-Driven Head and Neck Cancer-Striking the Balance Between Toxicity and Cure
Abstract
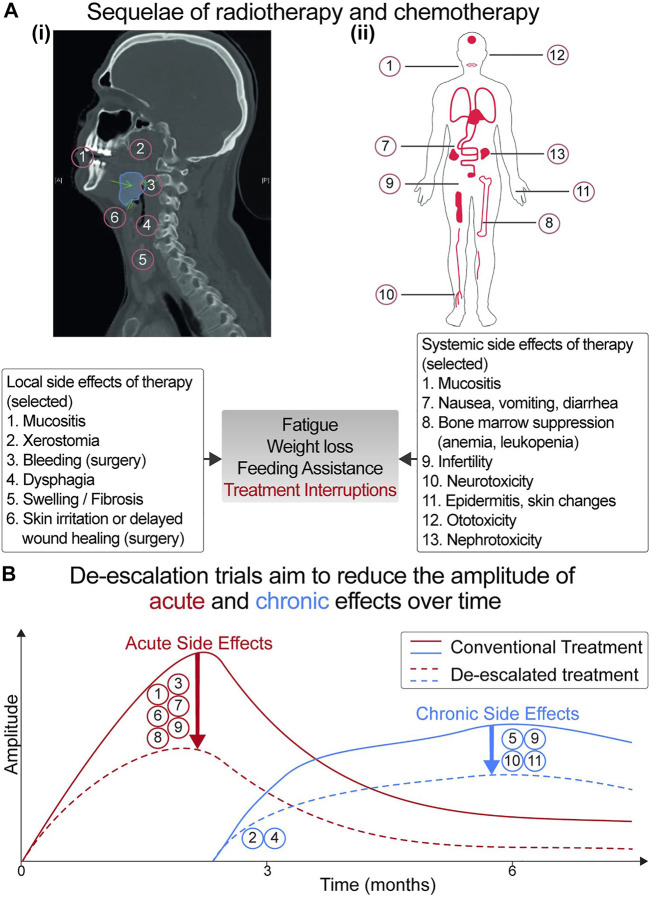
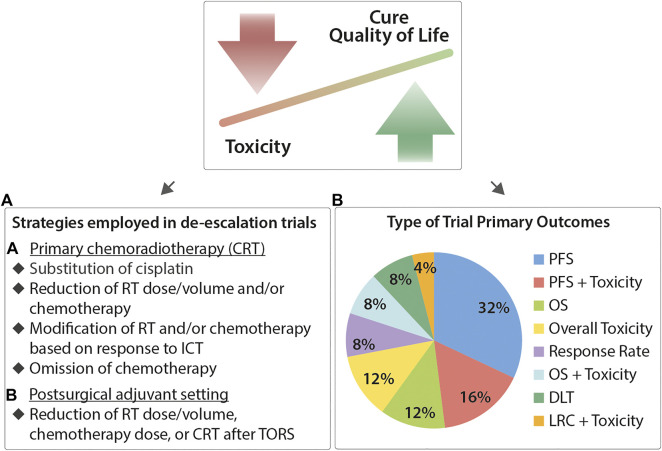
More than a decade after the discovery of p16 immunohistochemistry (IHC) as a surrogate for human papilloma virus (HPV)-driven head and neck squamous cell carcinoma (HNSCC), p16-IHC has become a routinely evaluated biomarker to stratify oropharyngeal squamous cell carcinoma (OPSCC) into a molecularly distinct subtype with favorable clinical prognosis. Clinical trials of treatment de-escalation frequently use combinations of biomarkers (p16-IHC, HPV-RNA in situ hybridization, and amplification of HPV-DNA by PCR) to further improve molecular stratification. Implementation of these methods into clinical routine may be limited in the case of RNA by the low RNA quality of formalin-fixed paraffin-embedded tissue blocks (FFPE) or in the case of DNA by cross contamination with HPV-DNA and false PCR amplification errors. Advanced technological developments such as investigation of tumor mutational landscape (NGS), liquid-biopsies (LBx and cell-free cfDNA), and other blood-based HPV immunity surrogates (antibodies in serum) may provide novel venues to further improve diagnostic uncertainties. Moreover, the value of HPV/p16-IHC outside the oropharynx in HNSCC patients needs to be clarified. With regards to therapy, postoperative (adjuvant) or definitive (primary) radiochemotherapy constitutes cornerstones for curative treatment of HNSCC. Side effects of chemotherapy such as bone-marrow suppression could lead to radiotherapy interruption and may compromise the therapy outcome. Therefore, reduction of chemotherapy or its replacement with targeted anticancer agents holds the promise to further optimize the toxicity profile of systemic treatment. Modern radiotherapy gradually adapts the dose. Higher doses are administered to the visible tumor bulk and positive lymph nodes, while a lower dose is prescribed to locoregional volumes empirically suspected to be invaded by tumor cells. Further attempts for radiotherapy de-escalation may improve acute toxicities, for example, the rates for dysphagia and feeding tube requirement, or ameliorate late toxicities like tissue scars (fibrosis) or dry mouth. The main objective of current de-intensification trials is therefore to reduce acute and/or late treatment-associated toxicity while preserving the favorable clinical outcomes. Deep molecular characterization of HPV-driven HNSCC and radiotherapy interactions with the tumor immune microenvironment may be instructive for the development of next-generation de-escalation strategies.
Keywords: de-intensification trials; head and neck (H&N) cancer; human papilloma virus—HPV; oropharyngeal cancer (OPC); patient stratification strategy; precision medicine; radiotherapy.
Copyright © 2022 Tawk, Debus and Abdollahi.
Conflict of interest statement
BT: None to report. JD: Research Grant; Siemens Health Care GmbH, Solution Akademia Gmbh, Viewray Inc., CRI The Clinical Research Institute GmbH, Accuray International Sari, RaySearch Laboratories AB, Vision RT Limited, Merck Serono GmbH, Astellas Pharma GmbH, Astra Zeneca GmbH, Egomed PLC Surrey Research Park, Quintiles GmbH, Pharmaceutical Research Associates Gm. AA: Research Grant; Merck KGaA, FibroGen, Bayer. Consulting or Advisory Role; Roche, Merck KGaA, Merck Serono, FibroGen, BMS Brazil, Bayer Health.
Figures
Similar articles
-
Clinico-pathological peculiarities of human papilloma virus driven head and neck squamous cell carcinoma: A comprehensive update.Life Sci. 2020 Mar 15;245:117383. doi: 10.1016/j.lfs.2020.117383. Epub 2020 Jan 30. Life Sci. 2020. PMID: 32007572 Review.
-
Challenges and Considerations in Diagnosing and Managing p16+-Related Oropharyngeal Squamous Cell Carcinoma (OPSCC) with Neck Metastasis: Implications of p16 Positivity, Tobacco Exposure, and De-Escalation Strategies.J Clin Med. 2024 Nov 11;13(22):6773. doi: 10.3390/jcm13226773. J Clin Med. 2024. PMID: 39597917 Free PMC article. Review.
-
Validation of local p16 testing for determination of human papilloma virus status eligibility on a low risk oropharyngeal cancer trial - A Trans-Tasman Radiation Oncology Group study.Oral Oncol. 2020 Nov;110:104988. doi: 10.1016/j.oraloncology.2020.104988. Epub 2020 Sep 1. Oral Oncol. 2020. PMID: 32889172
-
Optimizing Treatment De-Escalation in Head and Neck Cancer: Current and Future Perspectives.Oncologist. 2021 Jan;26(1):40-48. doi: 10.1634/theoncologist.2020-0303. Epub 2020 Sep 21. Oncologist. 2021. PMID: 32864799 Free PMC article. Review.
-
Human Papillomavirus DNA Detection by Droplet Digital PCR in Formalin-Fixed Paraffin-Embedded Tumor Tissue from Oropharyngeal Squamous Cell Carcinoma Patients.Mol Diagn Ther. 2021 Jan;25(1):59-70. doi: 10.1007/s40291-020-00502-6. Epub 2020 Nov 27. Mol Diagn Ther. 2021. PMID: 33245553
Cited by
-
Prevalence and genotype distribution of HPV infection among women in 2021-2023 in southern Iran: The rising trend of HPV infection among women.BMC Womens Health. 2025 Mar 20;25(1):126. doi: 10.1186/s12905-025-03668-5. BMC Womens Health. 2025. PMID: 40114128 Free PMC article.
-
Pharmacological impact of microRNAs in head and neck squamous cell carcinoma: Prevailing insights on molecular pathways, diagnosis, and nanomedicine treatment.Front Pharmacol. 2023 May 3;14:1174330. doi: 10.3389/fphar.2023.1174330. eCollection 2023. Front Pharmacol. 2023. PMID: 37205904 Free PMC article. Review.
-
[Phase II study on treatment de-escalation in HPV-associated oropharyngeal cancer].Strahlenther Onkol. 2022 Aug;198(8):755-758. doi: 10.1007/s00066-022-01948-9. Epub 2022 May 13. Strahlenther Onkol. 2022. PMID: 35552777 Free PMC article. Clinical Trial. German. No abstract available.
-
DNA-Methylome-Based Tumor Hypoxia Classifier Identifies HPV-Negative Head and Neck Cancer Patients at Risk for Locoregional Recurrence after Primary Radiochemotherapy.Clin Cancer Res. 2023 Aug 15;29(16):3051-3064. doi: 10.1158/1078-0432.CCR-22-3790. Clin Cancer Res. 2023. PMID: 37058257 Free PMC article.
-
TRIM21 Expression as a Prognostic Biomarker for Progression-Free Survival in HNSCC.Int J Mol Sci. 2023 Mar 7;24(6):5140. doi: 10.3390/ijms24065140. Int J Mol Sci. 2023. PMID: 36982215 Free PMC article.
References
-
- Adelstein D. J., Li Y., Adams G. L., Wagner H., Kish J. A., Ensley J. F., et al. (2003). An Intergroup Phase III Comparison of Standard Radiation Therapy and Two Schedules of Concurrent Chemoradiotherapy in Patients with Unresectable Squamous Cell Head and Neck Cancer. J. Clin. Oncol. 21, 92–98. 10.1200/JCO.2003.01.008 - DOI - PubMed
-
- Balermpas P., Rödel F., Rödel C., Krause M., Linge A., Lohaus F., et al. (2016). CD8+ Tumour-Infiltrating Lymphocytes in Relation to HPV Status and Clinical Outcome in Patients with Head and Neck Cancer after Postoperative Chemoradiotherapy: A Multicentre Study of the German Cancer Consortium Radiation Oncology Group (DKTK-ROG). Int. J. Cancer 138, 171–181. 10.1002/ijc.29683 - DOI - PubMed
-
- Beaty B., Gupta G. P., Shen C., Amdur R. J., Weiss J., Grilley-Olson J., et al. (2019). PIK3CA Mutation Is an Adverse Prognostic Factor in HPV-Associated Oropharynx Cancer. J Natl Cancer Inst. 105, S215. 10.1016/j.ijrobp.2019.06.295 - DOI
Publication types
LinkOut - more resources
Full Text Sources