

Family resilience and childhood obesity among children exposed to adverse childhood experiences in a national survey
- PMID: 35127118
- PMCID: PMC8804940
- DOI: 10.1002/osp4.497
Family resilience and childhood obesity among children exposed to adverse childhood experiences in a national survey
Abstract
Objective: Adverse childhood experiences (ACEs) contribute to poor overall health among children with obesity. This study evaluated how one potential protective factor-family resilience-affects the association between ACEs and childhood obesity.
Methods: This analysis was a secondary analysis of the 2016-2018 National Survey of Children's Health (NSCH), a repeated cross-sectional survey based on parent report. Nine ACEs were queried. Family resilience was assessed with four items (potential range 0-12). The primary outcome was child weight status. Multivariable ordinal logistic regression was used, adjusting for potential confounders and the interaction between ACEs and family resilience.
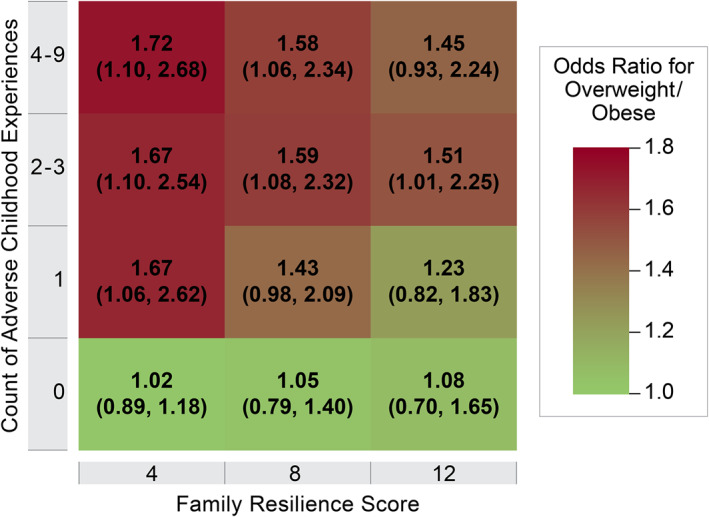
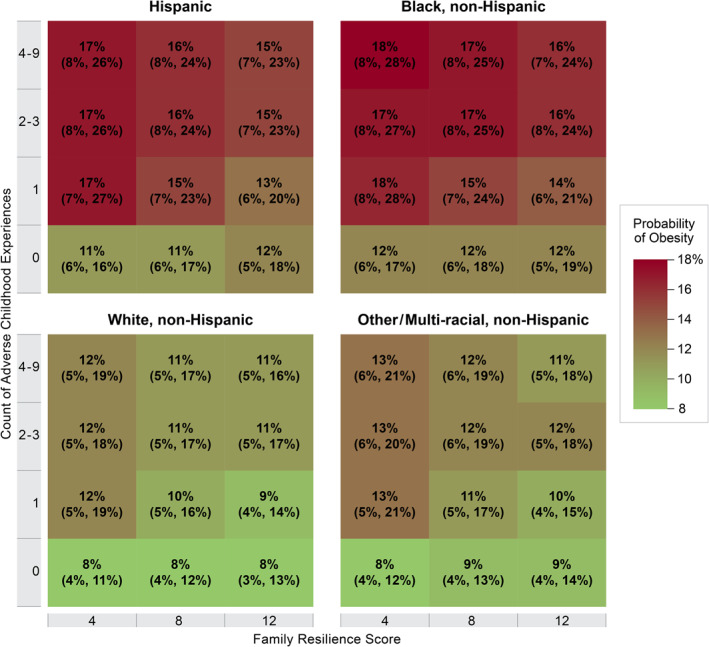
Results: For 49,365 children ages 10-17, the median number of ACEs was 1 (IQR 0, 2), the median family resilience score was 10 (IQR 8,12), 15.3% of children had overweight, and 15.4% of children had obesity. Among the 51.3% of children who experienced one or more ACEs, higher family resilience scores attenuated the odds of being in a higher weight category. This pattern was not observed in children with zero ACEs.
Conclusions: In the 2016-2018 NSCH, children ages 10-17 who were exposed to ACEs had higher rates of overweight and obesity, the odds of which may be reduced when children also have higher family resilience.
Keywords: adverse childhood experiences; childhood obesity; family resilience.
© 2021 The Authors. Obesity Science & Practice published by World Obesity and The Obesity Society and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Iguacel I, Gasch‐Gallén Á, Ayala‐Marín AM, De Miguel‐Etayo P, Moreno LA. Social vulnerabilities as risk factor of childhood obesity development and their role in prevention programs. Int J Obes (Lond). 2020;45(1):1‐11. - PubMed
-
- Lynch BA, Agunwamba A, Wilson PM, et al. Adverse family experiences and obesity in children and adolescents in the United States. Prev Med. 2016;90:148‐154. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources