

doi: 10.1016/j.eats.2021.08.029.
eCollection 2022 Jan.
Patellar Tendon Imbrication for Patella Alta
Affiliations
- PMID: 35127423
- PMCID: PMC8807527
- DOI: 10.1016/j.eats.2021.08.029
Item in Clipboard
Patellar Tendon Imbrication for Patella Alta
Arthrosc Tech.
.
Abstract
Patella alta is a significant contributor to patellar instability. Historically, distalizing tibial tubercle osteotomy has been recommended for this problem; however, complications such as nonunion, fracture and hardware irritation are concerning. Additionally, the procedure cannot be performed on skeletally immature patients without violation of the proximal tibial physis. The authors describe a technique of patellar tendon imbrication that does not involve hardware or osteotomy. This technique allows for reliable correction of patella alta and provides patellar stability without the complications associated with osteotomy.
© 2021 by the Arthroscopy Association of North America. Published by Elsevier.
Figures

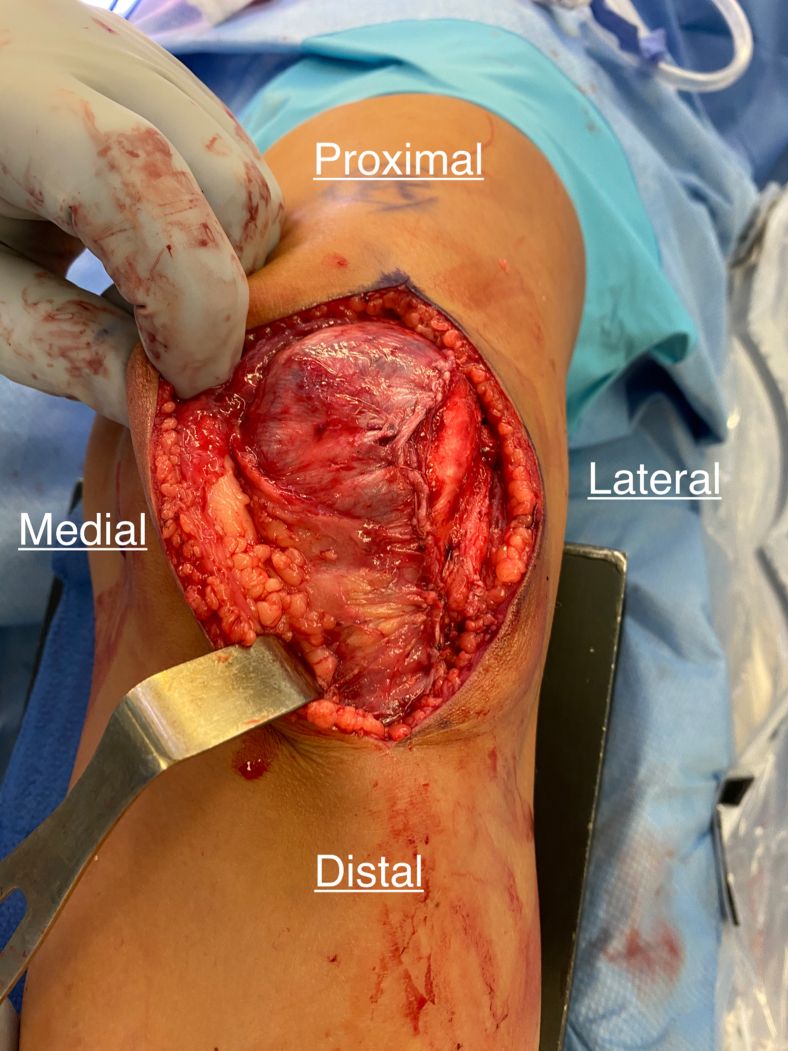
Patient is positioned supine with leg on radiolucent triangle in approximately 45°of flexion. Note the planned lateral para patellar incision.

After exposing the patella tendon, lines are drawn to demarcate the anticipated shortening. The most distal line is where the anterior tendon elevation will begin. The next line proximal is where the anterior flap elevation will end. In this example, this distance is 1 cm. The most proximal line is where the anchor point for the posterior pleat will be. That distance is half of the total length of the imbrication, which in this example is 5 mm.

The anterior 50% of the patellar tendon has been elevated. A fourth mark is now created on the intact posterior half of the tendon that is midway between the initiation and proximal terminus of flap elevation. Solid white line indicates the remaining posterior 50% of the patellar tendon.

Using 0-Vicryl suture (shown here in purple), a full-thickness pass is made through the proximal line and emerging at the midpoint of the intact posterior half of the tendon. A rip stop Mason-Allen type configuration is used distally before completing the mattress stitch. Not pictured here is the use of a broad osteotome that is used to stabilize the tendon and prevent inadvertent passage of sutures through the fat pad posterior to the tendon.

Nonabsorbable high-strength suture is then used to pass a mattress stich starting at the proximal end of the flap and ending at the beginning of flap elevation. A rip-stop configuration is used here as well, and it should be noted that this suture is kept anterior to the intact posterior half of the tendon when passing from proximal to distal. In this picture, an Army-Navy retractor (solid white arrow) is used to keep tension on the tendon to aid in suture passage, but it is now the author’s preference to use a broad osteotome deep into the tendon.

Once all sutures are passed but untied, tension is placed on the sutures, pulling the 0-Vicryl sutures (purple) proximally and the nonabsorbable sutures distally to approximate the imbrication.

Sutures are tied sequentially beginning with the 0-Vicryl sutures (purple) first followed by the nonabsorbable sutures. Imbrication is evaluated for stability through 90° of motion.
The laterally based elevation of the peritenon is closed over the imbricated tendon. In this picture, the lateral retinaculum was also closed in a lengthened fashion.
References
-
- Simmons E., Cameron J.C. Patella alta and recurrent dislocation of the patella. Clin Orthop Relat Res. 1992;(274):265–269. http://www.ncbi.nlm.nih.gov/pubmed/1729011 - PubMed
-
- Larsen E., Lauridsen F. Conservative treatment of patellar dislocations. Influence of evident factors on the tendency to redislocation and the therapeutic result. Clin Orthop Relat Res. 1982;(171):131–136. http://www.ncbi.nlm.nih.gov/pubmed/7140059 - PubMed
LinkOut - more resources
Full Text Sources
