

Therapy Trial Design in Vanishing White Matter: An Expert Consortium Opinion
- PMID: 35128050
- PMCID: PMC8811717
- DOI: 10.1212/NXG.0000000000000657
Therapy Trial Design in Vanishing White Matter: An Expert Consortium Opinion
Abstract
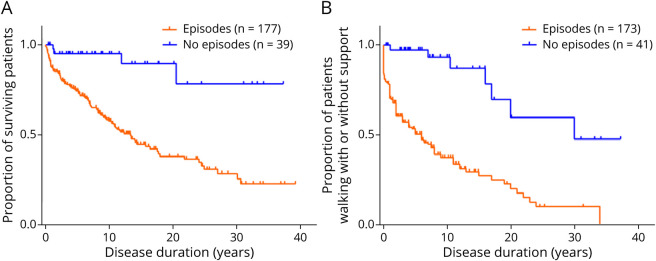
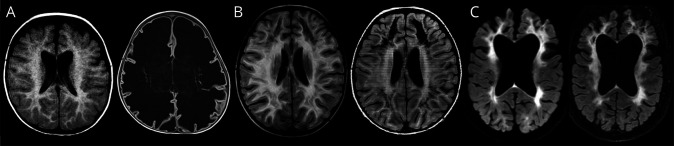
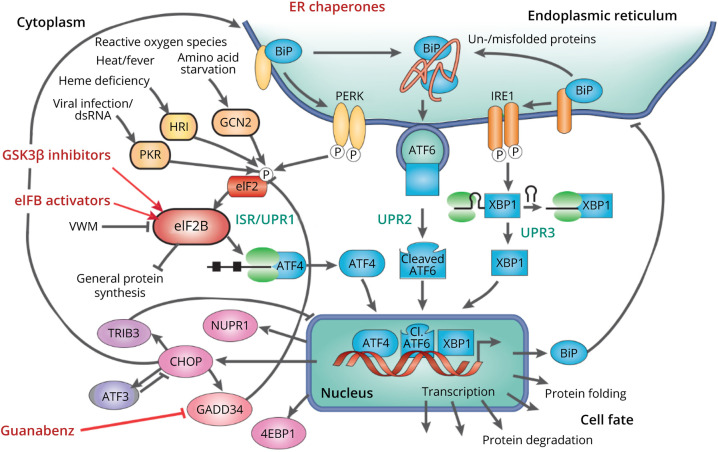
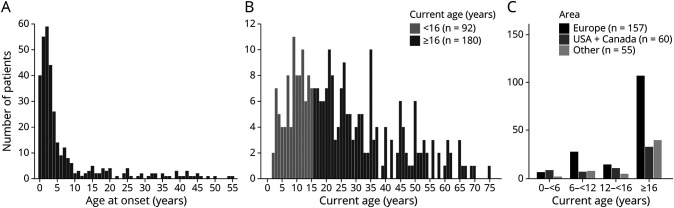
Vanishing white matter (VWM) is a leukodystrophy caused by recessive variants in the genes EIF2B1-EIF2B5. It is characterized by chronic neurologic deterioration with superimposed stress-provoked episodes of rapid decline. Disease onset spans from the antenatal period through senescence. Age at onset predicts disease evolution for patients with early onset, whereas disease evolution is unpredictable for later onset; patients with infantile and early childhood onset consistently have severe disease with rapid neurologic decline and often early death, whereas patients with later onset have highly variable disease. VWM is rare, but likely underdiagnosed, particularly in adults. Apart from measures to prevent stressors that could provoke acute deteriorations, only symptomatic care is currently offered. With increased insight into VWM disease mechanisms, opportunities for treatment have emerged. EIF2B1-EIF2B5 encode the 5-subunit eukaryotic initiation factor 2B complex, which is essential for translation of mRNAs into proteins and is a principal regulator of the integrated stress response (ISR). ISR deregulation is central to VWM pathology. Targeting components of the ISR has proven beneficial in mutant VWM mouse models, and several drugs are now in clinical development. However, clinical trials in VWM pose considerable challenges: low numbers of known patients with VWM, unpredictable disease course for patients with onset after early childhood, absence of intermediate biomarkers, and novel first-in-human molecular targets. Given these challenges and considering the critical need to offer therapies, we have formulated recommendations for enhanced diagnosis, drug trial setup, and patient selection, based on our expert evaluation of molecular, laboratory, and clinical data.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures

References
-
- Hanefeld F, Holzbach U, Kruse B, Wilichowski E, Christen HJ, Frahm J. Diffuse white matter disease in three children: an encephalopathy with unique features on magnetic resonance imaging and proton magnetic resonance spectroscopy. Neuropediatrics. 1993;24(5):244-248. - PubMed
-
- Schiffmann R, Moller JR, Trapp BD, et al. Childhood ataxia with diffuse central nervous system hypomyelination. Ann Neurol. 1994;35(3):331-340. - PubMed
-
- van der Knaap MS, Barth PG, Gabreëls FJ, et al. A new leukoencephalopathy with vanishing white matter. Neurology. 1997;48(4):845-855. - PubMed
-
- Leegwater PA, Vermeulen G, Könst AA, et al. Subunits of the translation initiation factor eIF2B are mutant in leukoencephalopathy with vanishing white matter. Nat Genet. 2001;29(4):383-388. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources