

Fecal Incontinence: The Importance of a Structured Pathophysiological Model
- PMID: 35128138
- PMCID: PMC8801252
- DOI: 10.23922/jarc.2021-040
Fecal Incontinence: The Importance of a Structured Pathophysiological Model
Abstract
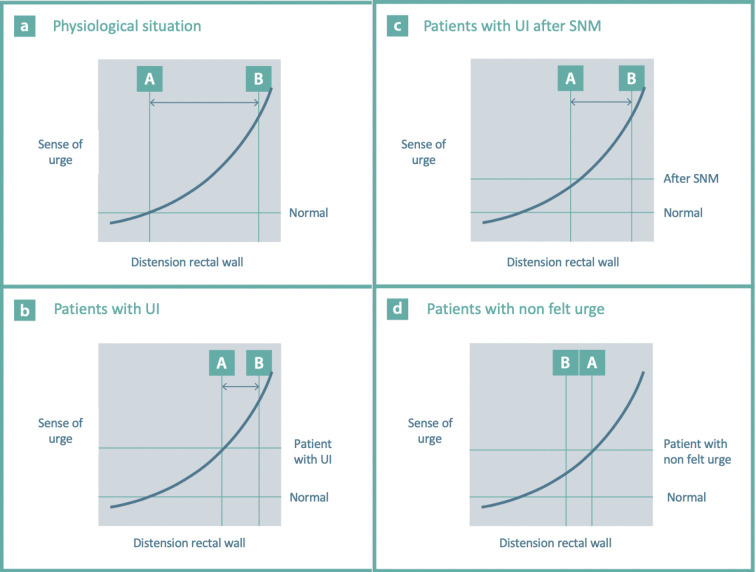
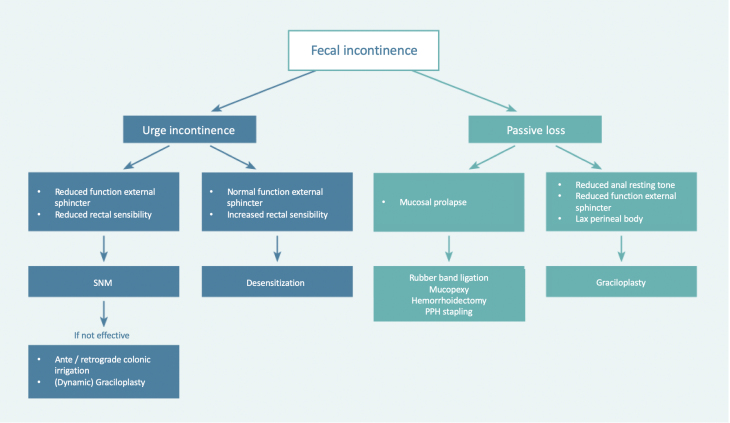
Fecal incontinence has an enormous social and economic impact and may significantly impair quality of life. Even though fecal incontinence is a common complaint in (aging) adults, a structured pathophysiological model of the clinical presentations of fecal incontinence is missing in current literature. The most frequent manifestations of fecal incontinence are passive fecal loss, urge incontinence, or mixed fecal incontinence. At our institution, we treat 400 patients per year with defecation disorders, including a significant number of patients with fecal incontinence. On the basis of this experience, we have tried to create a concept that merges current insight in causes and treatment options in a clinically useful algorithm. By applying the system of anamnesis and physical examination described in this article and expanding it with simple additional anorectal examination, in most patients, one can determine the type of fecal incontinence and choose a targeted therapy.
Keywords: fecal incontinence; gastroenterology; graciloplasty; proctology; sacral neuromodulation; surgery.
Copyright © 2022 by The Japan Society of Coloproctology.
Conflict of interest statement
Conflicts of Interest There are no conflicts of interest.
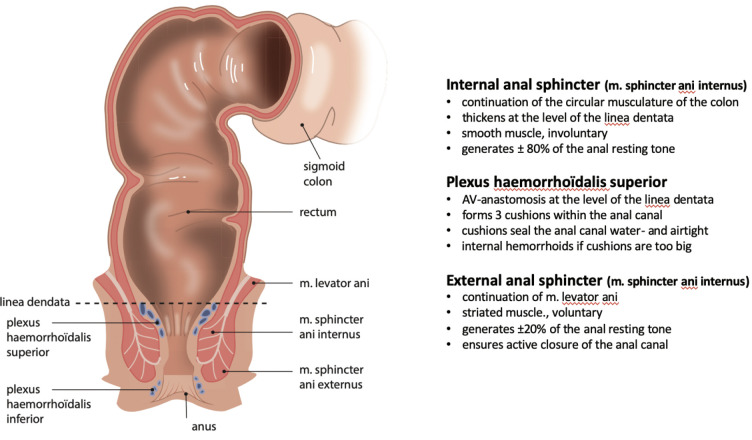
Figures
References
-
- Ng KS, Sivakumaran Y, Nassar N, et al. Fecal incontinence: Community prevalence and associated factors - A systematic review. Diseases of the colon and rectum 2015 Dec; 58(12): 1194-209. - PubMed
-
- Bharucha AE, Zinsmeister AR, Locke GR, et al. Prevalence and burden of fecal incontinence: A population-based study in women. Gastroenterology 2005 Jul; 129(1): 42-9. - PubMed
-
- Maeda K, Yamana T, Takao Y, et al. Japanese Practice Guidelines for Fecal Incontinence Part 1 - Definition, epidemiology, etiology, pathophysiology and causes, risk factors, clinical evaluations, and symptomatic scores and QoL questionnaire for clinical evaluations - English version. Journal of the Anus, Rectum and Colon. 2021 Jan; 5(1): 52-66. - PMC - PubMed