

Rapid vigilance and episodic memory decrements in COVID-19 survivors
- PMID: 35128398
- PMCID: PMC8807287
- DOI: 10.1093/braincomms/fcab295
Rapid vigilance and episodic memory decrements in COVID-19 survivors
Abstract
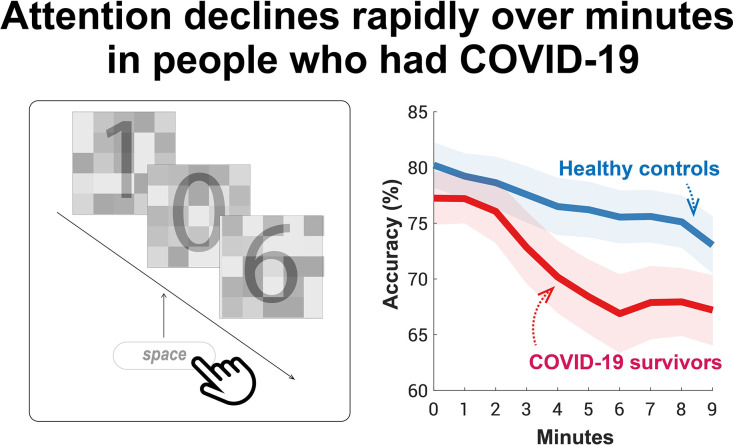
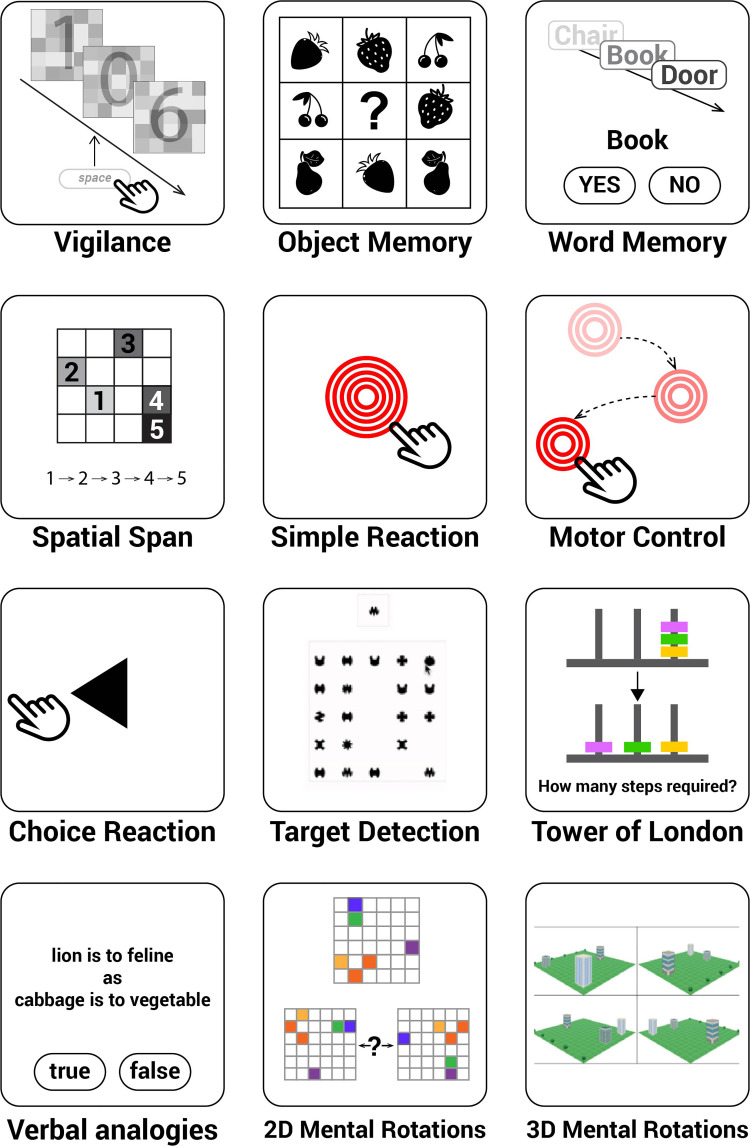
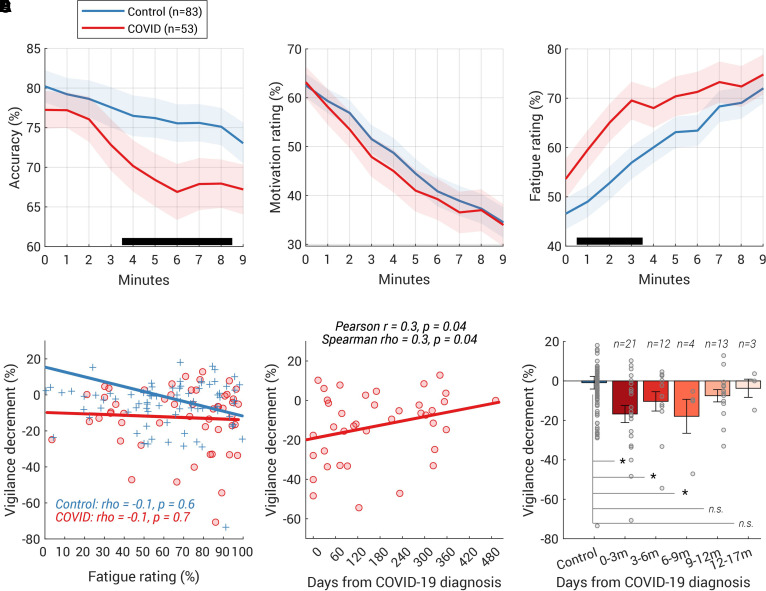
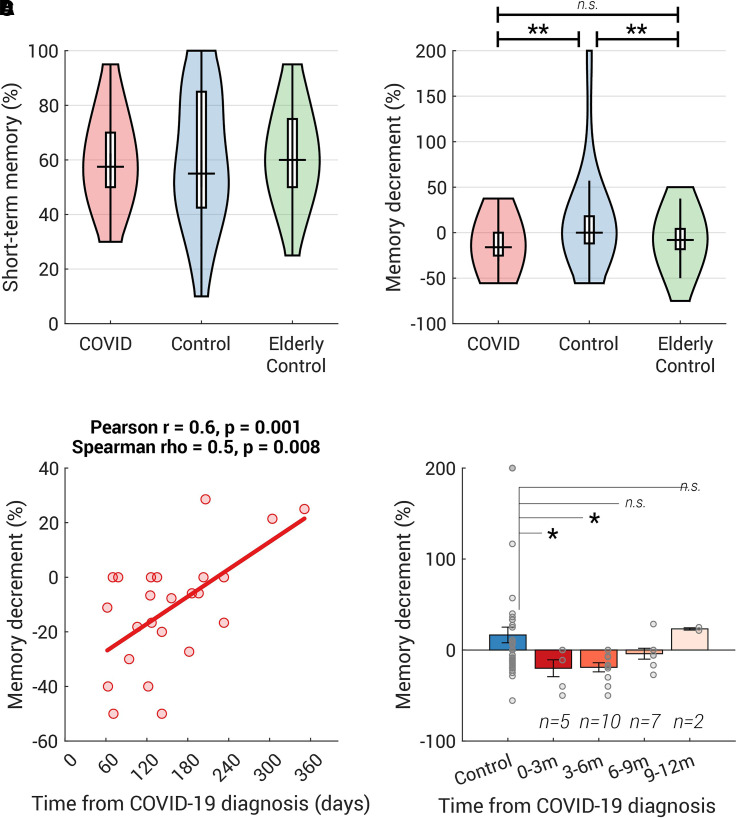
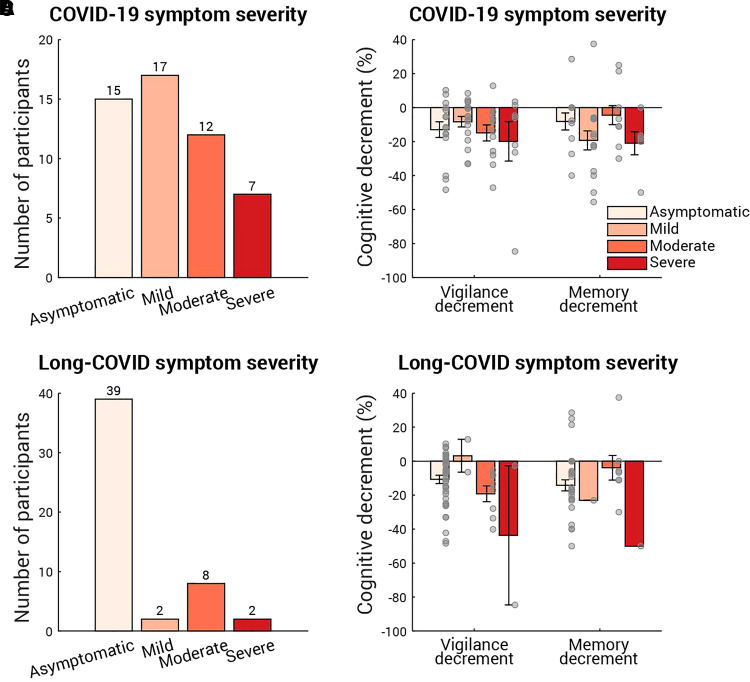
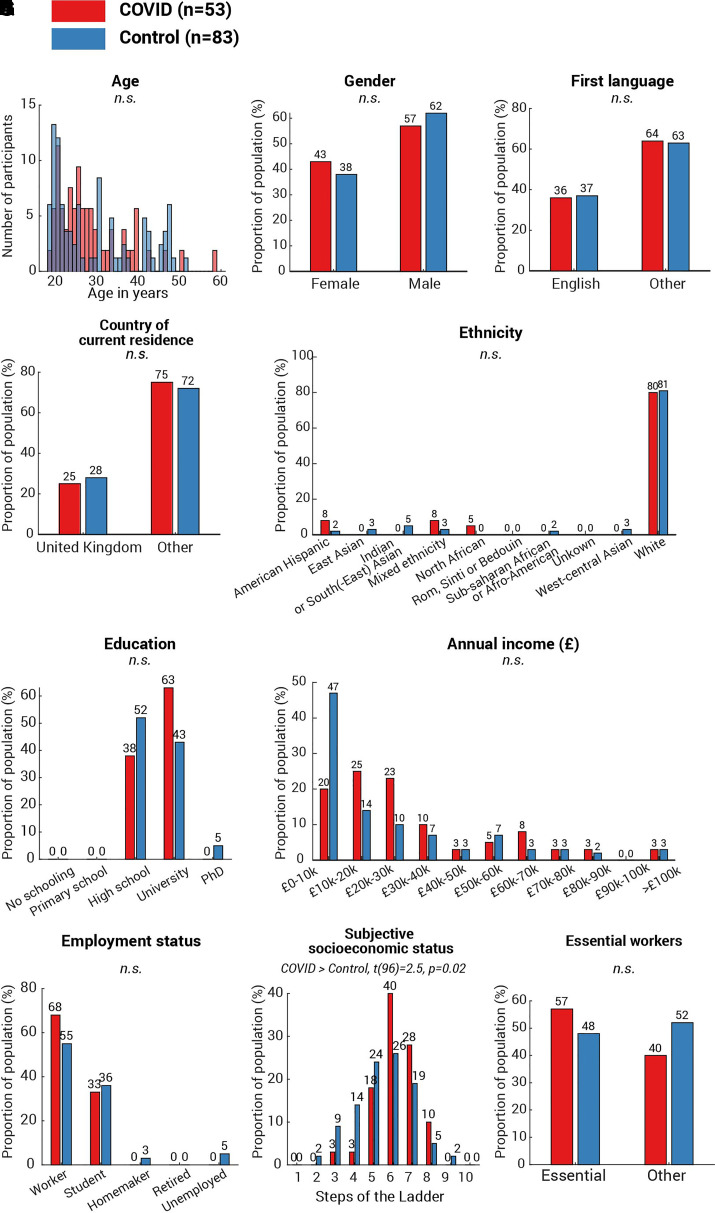
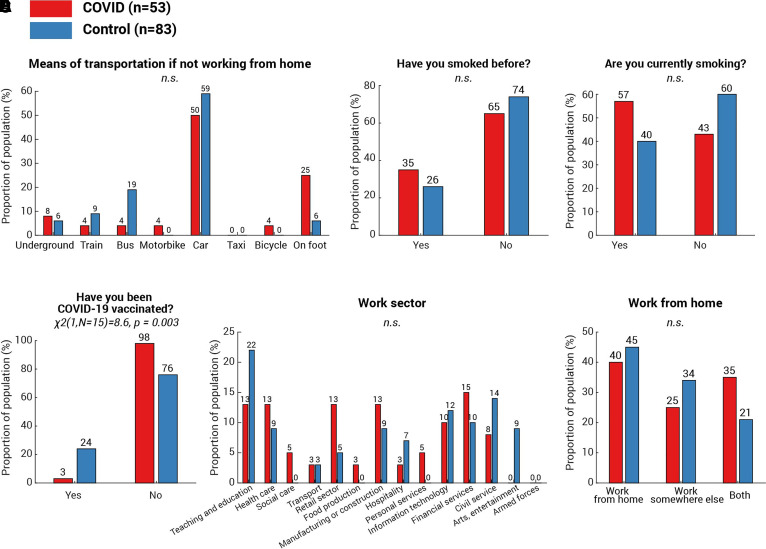
Recent studies indicate that COVID-19 infection can lead to serious neurological consequences in a small percentage of individuals. However, in the months following acute illness, many more suffer from fatigue, low motivation, disturbed mood, poor sleep and cognitive symptoms, colloquially referred to as 'brain fog'. But what about individuals who had asymptomatic to moderate COVID-19 and reported no concerns after recovering from COVID-19? Here, we examined a wide range of cognitive functions critical for daily life (including sustained attention, memory, motor control, planning, semantic reasoning, mental rotation and spatial-visual attention) in people who had previously suffered from COVID-19 but were not significantly different from a control group on self-reported fatigue, forgetfulness, sleep abnormality, motivation, depression, anxiety and personality profile. Reassuringly, COVID-19 survivors performed well in most abilities tested, including working memory, executive function, planning and mental rotation. However, they displayed significantly worse episodic memory (up to 6 months post-infection) and greater decline in vigilance with time on task (for up to 9 months). Overall, the results show that specific chronic cognitive changes following COVID-19 are evident on objective testing even amongst those who do not report a greater symptom burden. Importantly, in the sample tested here, these were not significantly different from normal after 6-9 months, demonstrating evidence of recovery over time.
Keywords: COVID-19; cognitive deficits; long-COVID; memory; sustained attention.
© The Author(s) (2022). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical