

The inadequate corpus luteum
- PMID: 35128435
- PMCID: PMC8812462
- DOI: 10.1530/RAF-20-0044
The inadequate corpus luteum
Abstract
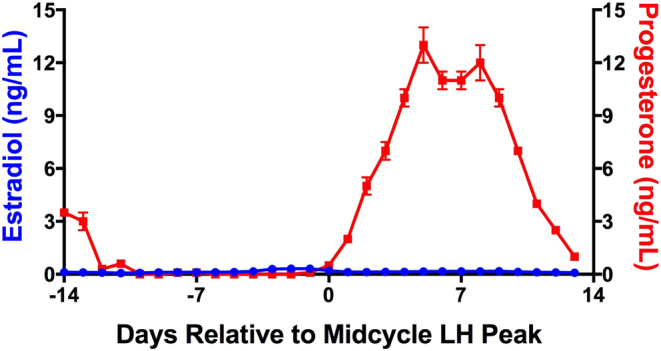
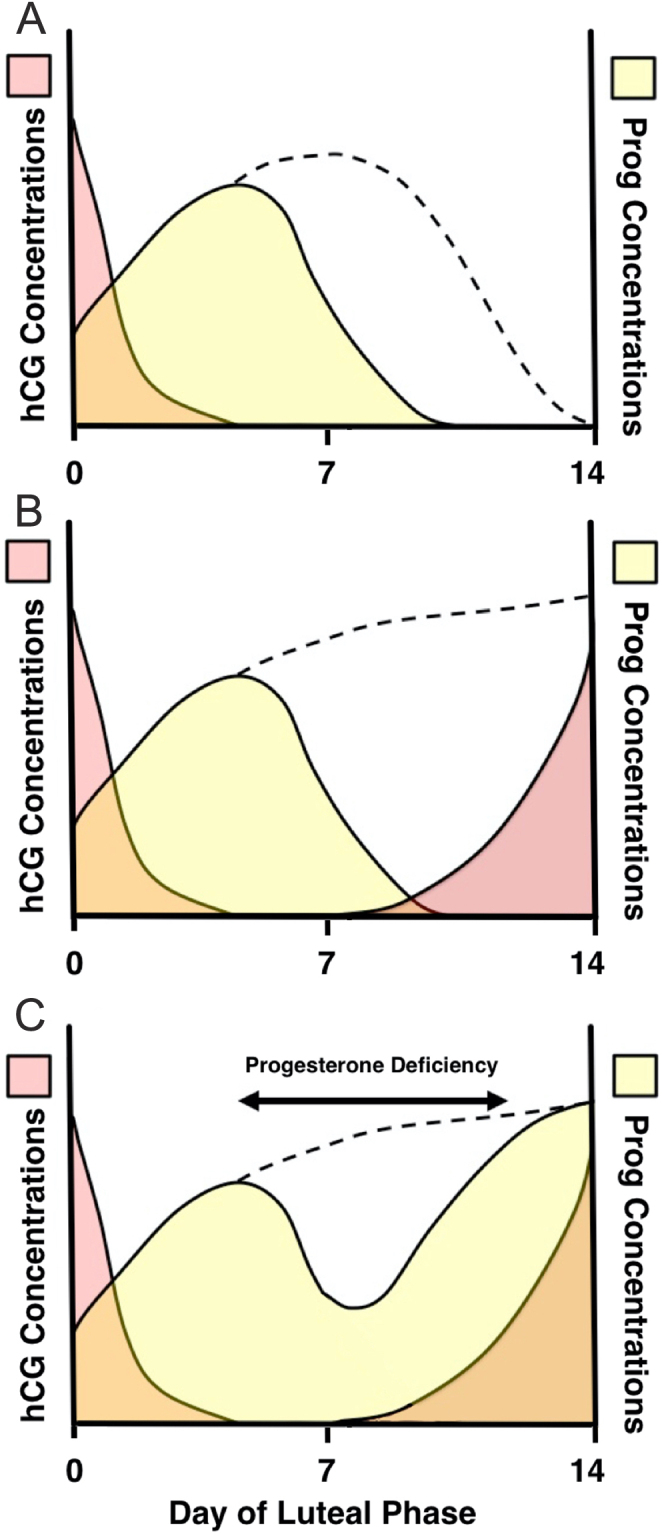
The corpus luteum is the source of progesterone in the luteal phase of the cycle and the initial two-thirds of the first trimester of pregnancy. Normal luteal function is required for fertility and the maintenance of pregnancy. Progesterone administration is increasingly used during fertility treatments and in early pregnancy to mitigate potentially inadequate corpus luteum function. This commentary considers the concept of the inadequate corpus luteum and the role and effects of exogenous progesterone. Progesterone supplementation does have important beneficial effects but we should be wary of therapeutic administration beyond or outside the evidence base.
Lay summary: After an egg is released a structure is formed on the ovary called a corpus luteum (CL). This produces a huge amount of a hormone called progesterone. Progesterone makes the womb ready for pregnancy but if a pregnancy does not happen the CL disappears after 12-14 days and this causes a period. If a pregnancy occurs, then the pregnancy hormone (hCG) keeps the CL alive and its progesterone supports the pregnancy for the next 6-8 weeks until the placenta takes over and the corpus luteum disappears. That means that if the CL is not working correctly there could be problems getting pregnant or staying pregnant. If a CL is not producing enough progesterone it usually means there is a problem with the growing or releasing of the egg and treatment should focus on these areas. In IVF cycles, where normal hormones are switched off, the CL does not produce quite enough progesterone before the pregnancy test and extra progesterone is needed at this time. In recurrent or threatened miscarriage, however, there is not any evidence that the CL is not working well or progesterone is low. However, there is benefit in taking extra progesterone if there is bleeding in early pregnancy in women with previous miscarriages. This might be because of the effects of high-dose progesterone on the womb or immune system. As changes to the hormone environment in pregnancy may have some life-long consequences for the offspring we have to be careful only to give extra progesterone when we are sure it is needed.
Keywords: infertility; luteal phase defect; luteal support; miscarriage; progesterone.
© 2021 The authors.
Conflict of interest statement
The author declares that there is no conflict of interest that could be perceived as prejudicing the impartiality of this commentary.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
