

Postoperative Opioid Prescribing and New Persistent Opioid Use: The Risk of Excessive Prescribing
- PMID: 35129474
- PMCID: PMC10537242
- DOI: 10.1097/SLA.0000000000005392
Postoperative Opioid Prescribing and New Persistent Opioid Use: The Risk of Excessive Prescribing
Abstract
Objective: Evaluate the association between postoperative opioid prescribing and new persistent opioid use.
Summary background data: Opioid-nave patients who develop new persistent opioid use after surgery are at increased risk of opioid-related morbidity and mortality. However, the extent to which postoperative opioid prescribing is associated with persistent postoperative opioid use is unclear.
Methods: Retrospective study of opioid-naïve adults undergoing surgery in Michigan from 1/1/2017 to 10/31/2019. Postoperative opioid prescriptions were identified using a statewide clinical registry and prescription fills were identified using Michigan's prescription drug monitoring program. The primary outcome was new persistent opioid use, defined as filling at least 1 opioid prescription between post-discharge days 4 to 90 and filling at least 1 opioid prescription between post-discharge days 91 to 180.
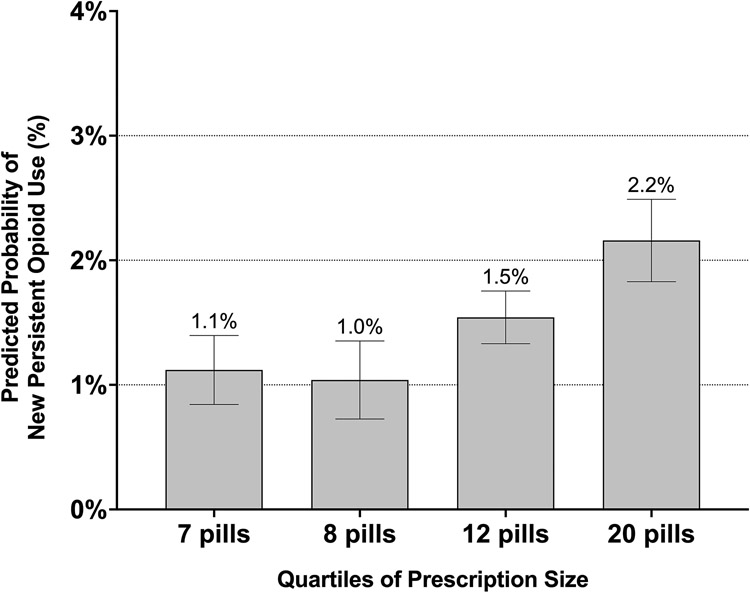
Results: A total of 37,654 patients underwent surgery with a mean age of 52.2 (16.7) years and 20,923 (55.6%) female patients. A total of 31,920 (84.8%) patients were prescribed opioids at discharge. Six hundred twenty-two (1.7%) patients developed new persistent opioid use after surgery. Being prescribed an opioid at discharge was not associated with new persistent opioid use [adjusted odds ratio (aOR) 0.88 (95% confidence interval (CI) 0.71-1.09)]. However, among patients prescribed an opioid, patients prescribed the second largest [12 (interquartile range (IQR) 3) pills] and largest [20 (IQR 7) pills] quartiles of prescription size had higher odds of new persistent opioid use compared to patients prescribed the smallest quartile [7 (IQR 1) pills] of prescription size [aOR 1.39 (95% CI 1.04-1.86) andaOR 1.97 (95% CI 1.442.70), respectively].
Conclusions: In a cohort of opioid-naïve patients undergoing common surgical procedures, the risk of new persistent opioid use increased with the size of the prescription. This suggests that while opioid prescriptions in and of themselves may not place patients at risk of long-term opioid use, excessive prescribing does. Consequently, these findings support ongoing efforts to mitigate excessive opioid prescribing after surgery to reduce opioid-related harms.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Waljee JF, Li L, Brummett CM, Englesbe MJ. Iatrogenic Opioid Dependence in the United States: Are Surgeons the Gatekeepers? Ann Surg. 2017;265(4):728–730. - PubMed
-
- Nelson DB, Cata JP, Niu J, et al. Persistent opioid use is associated with worse survival after lobectomy for stage I non-small cell lung cancer. Pain. 2019;160(10):2365–2373. - PubMed
