

Deaths in a Modern Cohort of Extremely Preterm Infants From the Preterm Erythropoietin Neuroprotection Trial
- PMID: 35129596
- PMCID: PMC8822378
- DOI: 10.1001/jamanetworkopen.2021.46404
Deaths in a Modern Cohort of Extremely Preterm Infants From the Preterm Erythropoietin Neuroprotection Trial
Abstract
Importance: Understanding why and how extremely preterm infants die is important for practitioners caring for these infants.
Objective: To examine risk factors, causes, timing, and circumstances of death in a modern cohort of extremely preterm infants.
Design, setting, and participants: A retrospective cohort review of infants enrolled in the Preterm Erythropoietin Neuroprotection Trial between December 13, 2013, and September 26, 2016, was conducted. A total of 941 infants born between 24 0/7 and 27 6/7 weeks of gestation enrolled at 19 US sites comprising 30 neonatal intensive care units were included. Data analysis was performed from October 16, 2020, to December 1, 2021.
Main outcomes and measures: Risk factors, proximal causes, timing, and circumstances of in-hospital death.
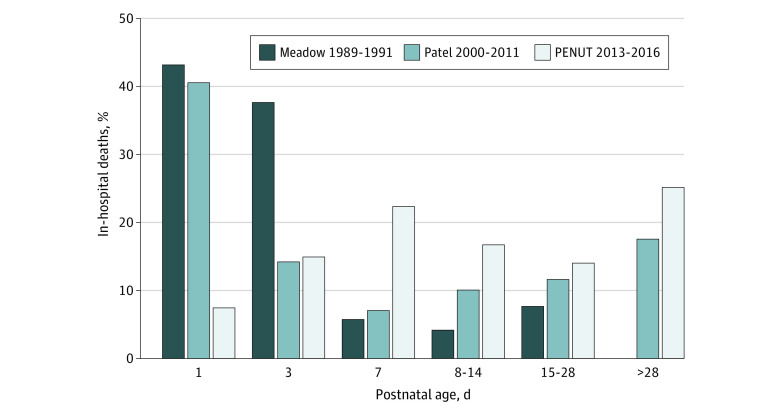
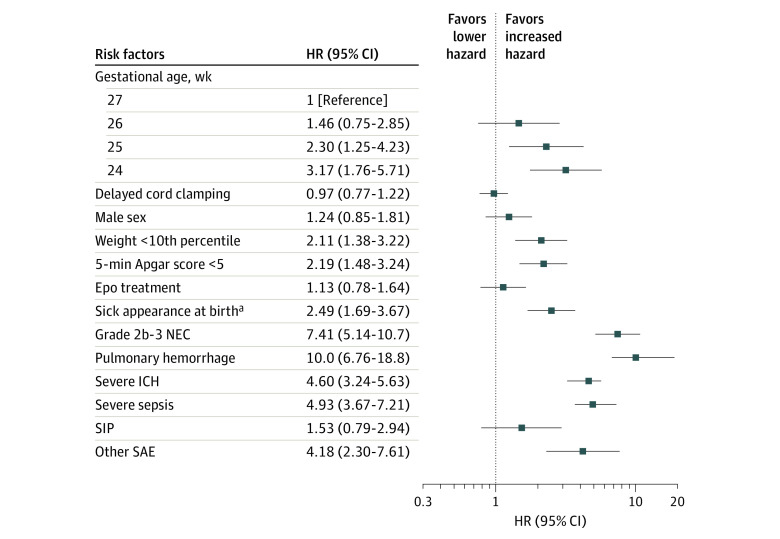
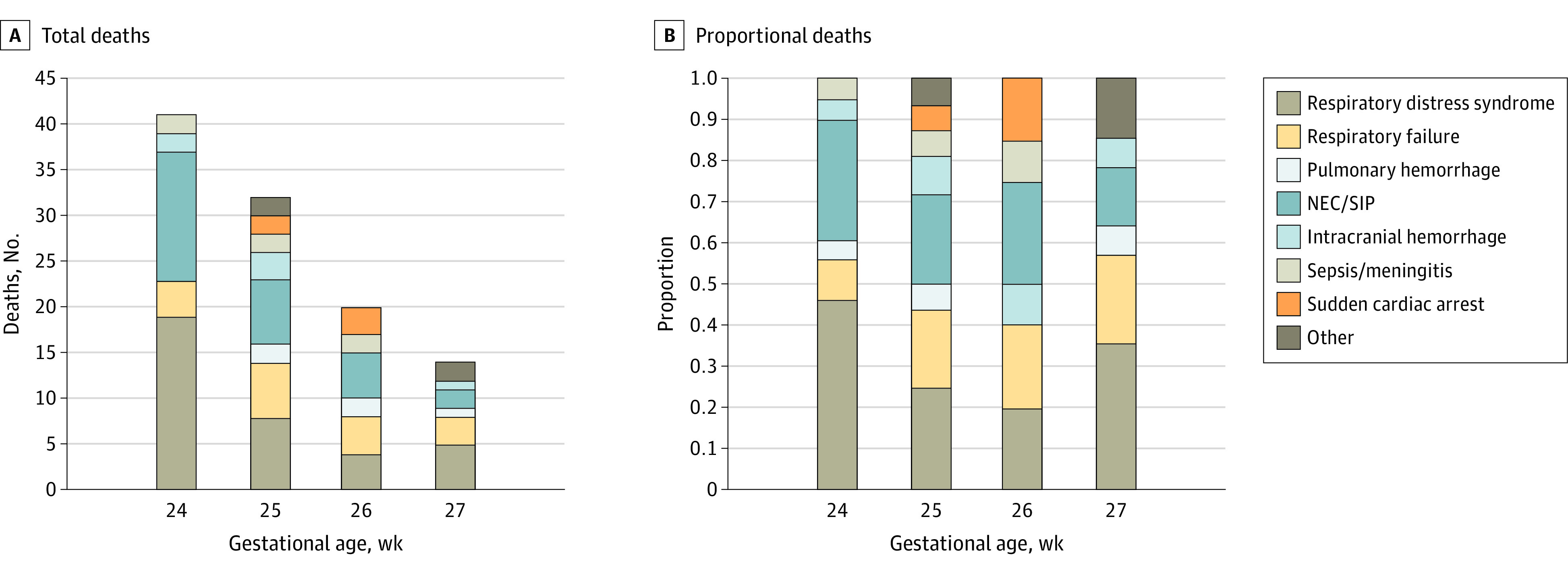
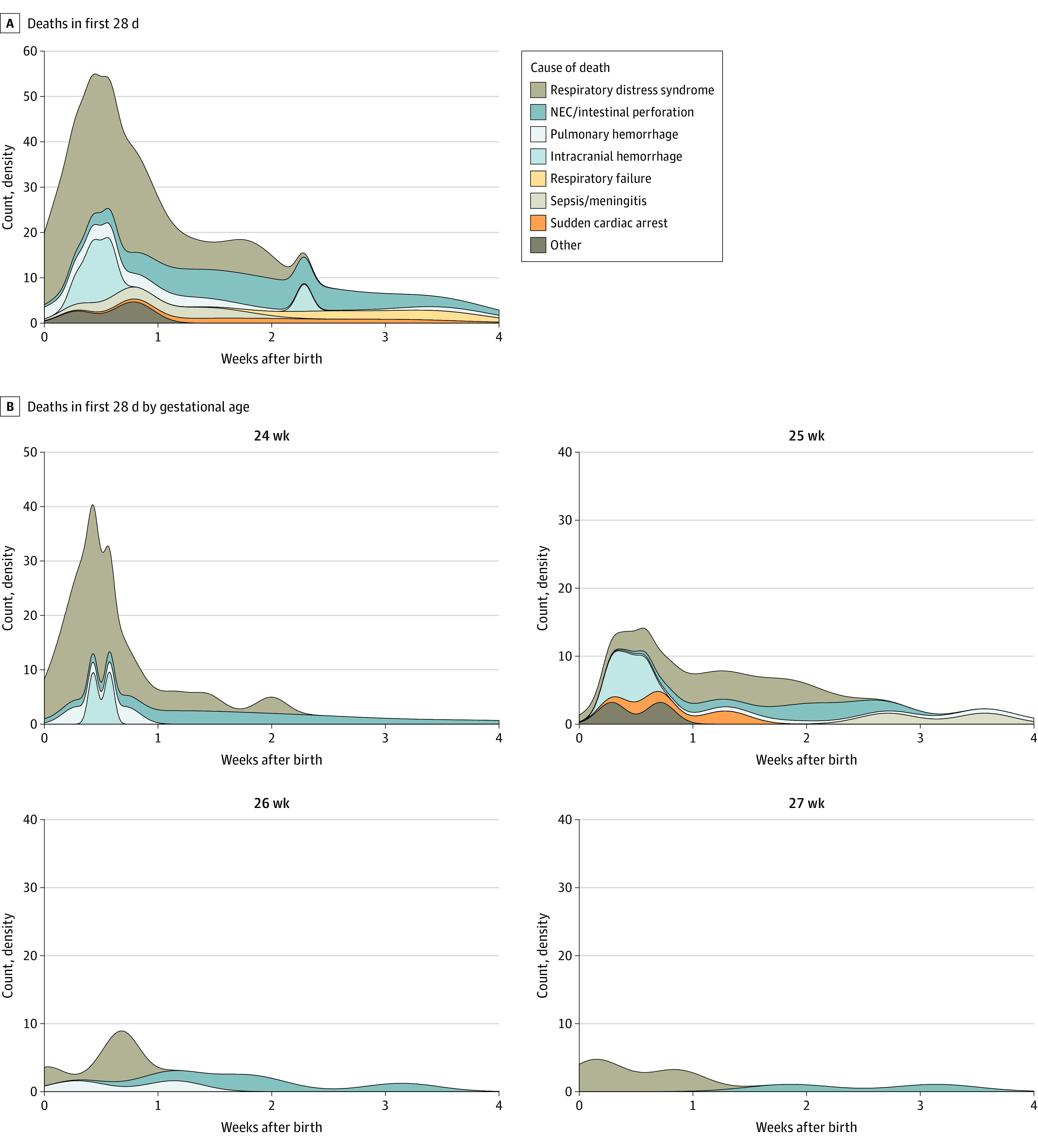
Results: Of the 941 enrolled infants, 108 died (11%) before hospital discharge: 38% (n = 41) at 24 weeks' gestation, 30% (n = 32) at 25 weeks' gestation, 19% (n = 20) at 26 weeks' gestation, and 14% (n = 15) at 27 weeks' gestation. An additional 9 infants (1%) died following hospital discharge. In descending order, the primary causes of death included respiratory distress or failure, pulmonary hemorrhage, necrotizing enterocolitis, catastrophic intracranial hemorrhage, sepsis, and sudden unexplained death. Fifty percent of deaths occurred within the first 10 days after birth. The risk of death decreased with day of life and postmenstrual age such that an infant born at 24 weeks' gestation who survived 14 days had the same risk of death as an infant born at 27 weeks' gestation: conditional proportional risk of death, 0.08 (95% CI, 0.03-0.13) vs 0.06 (95% CI, 0.01-0.11). Preterm labor was associated with a decreased hazard of death (hazard ratio [HR], 0.45; 95% CI, 0.31-0.66). Infant clinical factors associated with death included birth weight below the tenth percentile for gestational age (HR, 2.11; 95% CI, 1.38-3.22), Apgar score less than 5 at 5 minutes (HR, 2.19; 95% CI, 1.48-3.24), sick appearance at birth (HR, 2.49; 95% CI, 1.69-3.67), grade 2b-3 necrotizing enterocolitis (HR, 7.41; 95% CI, 5.14-10.7), pulmonary hemorrhage (HR, 10.0; 95% CI, 6.76-18.8), severe intracranial hemorrhage (HR, 4.60; 95% CI, 3.24-5.63), and severe sepsis (HR, 4.93; 95% CI, 3.67-7.21). Fifty-one percent of the infants received comfort care before death.
Conclusions and relevance: In this cohort study, an association between mortality and gestational age at birth was noted; however, for each week that an infant survived, their risk of subsequent death approximated the risk observed in infants born 1 to 2 weeks later, suggesting the importance of an infant's postmenstrual age. This information may be useful to include in counseling of families regarding prognosis of survival.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
