

Neuromodulation for Chronic Daily Headache
- PMID: 35129825
- PMCID: PMC8927000
- DOI: 10.1007/s11916-022-01025-x
Neuromodulation for Chronic Daily Headache
Abstract
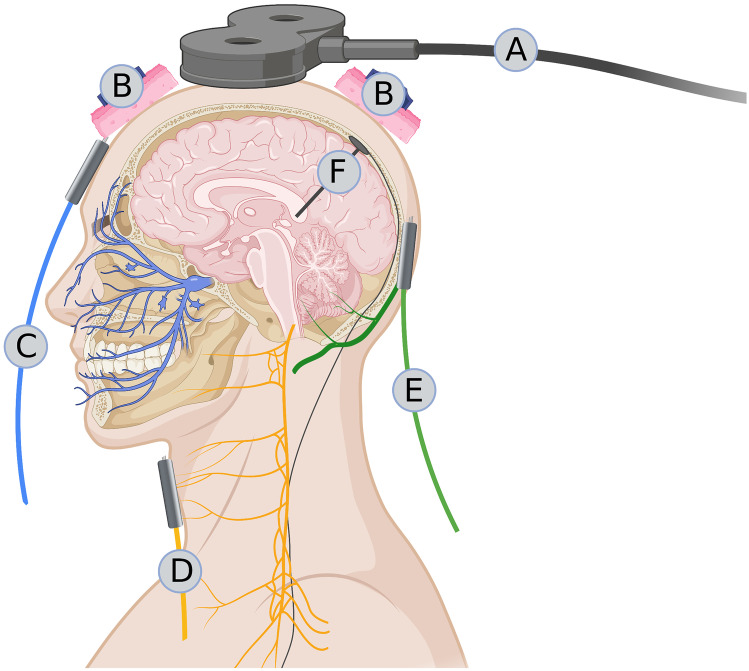
Purpose of review: We reviewed the literature that explored the use of central and peripheral neuromodulation techniques for chronic daily headache (CDH) treatment.
Recent findings: Although the more invasive deep brain stimulation (DBS) is effective in chronic cluster headache (CCH), it should be reserved for extremely difficult-to-treat patients. Percutaneous occipital nerve stimulation has shown similar efficacy to DBS and is less risky in both CCH and chronic migraine (CM). Non-invasive transcutaneous vagus nerve stimulation is a promising add-on treatment for CCH but not for CM. Transcutaneous external trigeminal nerve stimulation may be effective in treating CM; however, it has not yet been tested for cluster headache. Transcranial magnetic and electric stimulations have promising preventive effects against CM and CCH. Although the precise mode of action of non-invasive neuromodulation techniques remains largely unknown and there is a paucity of controlled trials, they should be preferred to more invasive techniques for treating CDH.
Keywords: Deep brain stimulation; Direct current stimulation; Occipital nerve; Sphenopalatine ganglia; Transcranial magnetic stimulation; Trigeminal nerve; Vagus nerve.
© 2022. The Author(s).
Conflict of interest statement
G. C., F. C., G. S., C. A., E. C. C. D. L., and M. S. declare no conflict of interest related to the topic of the present manuscript. D. M. received research and travel grants from ElectroCore. She contributed to the study with the supraorbital device Cefaly Technology without any compensation. She took place to several advisory boards organised by Medtronic without any compensation. She kindly received support for training from Theranica Bio-Electronics Ltd without any compensation.
Figures
References
-
- Cameron C, Kelly S, Hsieh SC, Murphy M, Chen L, Kotb A, et al. Triptans in the acute treatment of migraine: a systematic review and network meta-analysis. Headache. 2015;55(Suppl 4):221–235. - PubMed
-
- Thorlund K, Toor K, Wu P, Chan K, Druyts E, Ramos E, et al. Comparative tolerability of treatments for acute migraine: a network meta-analysis. Cephalalgia. 2017;37:965–978. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
