

Frailty Status Is a More Robust Predictor Than Age of Spinal Tumor Surgery Outcomes: A NSQIP Analysis of 4,662 Patients
- PMID: 35130424
- PMCID: PMC8987561
- DOI: 10.14245/ns.2142770.385
Frailty Status Is a More Robust Predictor Than Age of Spinal Tumor Surgery Outcomes: A NSQIP Analysis of 4,662 Patients
Abstract
Objective: The present study aimed to evaluate the effect of baseline frailty status (as measured by modified frailty index-5 [mFI-5]) versus age on postoperative outcomes of patients undergoing surgery for spinal tumors using data from a large national registry.
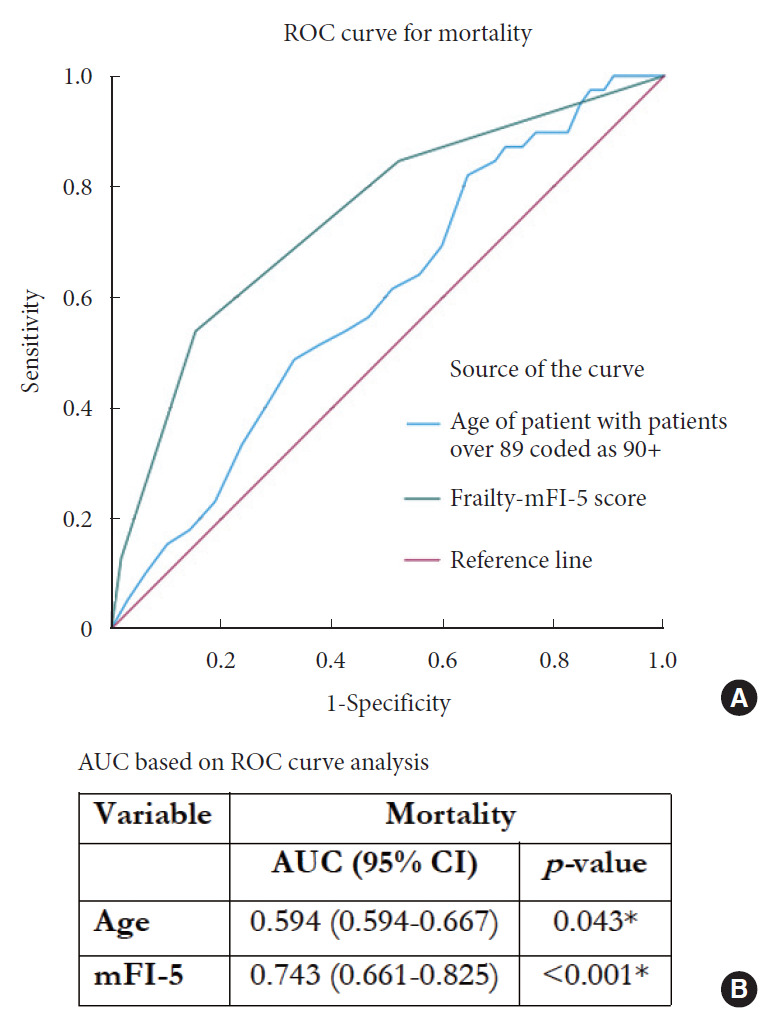
Methods: The National Surgical Quality Improvement Program database was used to collect spinal tumor resection patients' data from 2015 to 2019 (n = 4,662). Univariate and multivariate analyses for age and mFI-5 were performed for the following outcomes: 30-day mortality, major complications, unplanned reoperation, unplanned readmission, hospital length of stay (LOS), and discharge to a nonhome destination. Receiver operating characteristic (ROC) curve analysis was used to evaluate the discriminative performance of age versus mFI-5.
Results: Both univariate and multivariate analyses demonstrated that mFI-5 was a more robust predictor of worse postoperative outcomes as compared to age. Furthermore, based on categorical analysis of frailty tiers, increasing frailty was significantly associated with increased risk of adverse outcomes. 'Severely frail' patients were found to have the highest risk, with odds ratio 16.4 (95% confidence interval [CI],11.21-35.44) for 30-day mortality, 3.02 (95% CI, 1.97-4.56) for major complications, and 2.94 (95% CI, 2.32-4.21) for LOS. In ROC curve analysis, mFI-5 score (area under the curve [AUC] = 0.743) achieved superior discrimination compared to age (AUC = 0.594) for mortality.
Conclusion: Increasing frailty, as measured by mFI-5, is a more robust predictor as compared to age, for poor postoperative outcomes in spinal tumor surgery patients. The mFI-5 may be clinically used for preoperative risk stratification of spinal tumor patients.
Keywords: Age; Frailty; Modified frailty index-5; National Surgical Quality Improvement Project; Spinal tumors; Surgical outcomes.
Conflict of interest statement
The authors have nothing to disclose.
Figures

Comment in
-
Commentary on "Frailty Status Is a More Robust Predictor Than Age of Spinal Tumor Surgery Outcomes: A NSQIP Analysis of 4,662 Patients".Neurospine. 2022 Mar;19(1):63-64. doi: 10.14245/ns.2244110.055. Epub 2022 Mar 31. Neurospine. 2022. PMID: 35378582 Free PMC article. No abstract available.
Similar articles
-
The 5-item modified frailty index predicts spinal osteotomy outcomes better than age in adult spinal deformity patients: an ACS - NSQIP analysis.Spine Deform. 2023 Sep;11(5):1189-1197. doi: 10.1007/s43390-023-00712-y. Epub 2023 Jun 8. Spine Deform. 2023. PMID: 37291408
-
Association of baseline frailty status and age with outcomes in patients undergoing intracranial meningioma surgery: Results of a nationwide analysis of 5818 patients from the National Surgical Quality Improvement Program (NSQIP) 2015-2019.Eur J Surg Oncol. 2022 Jul;48(7):1671-1677. doi: 10.1016/j.ejso.2022.02.015. Epub 2022 Feb 11. Eur J Surg Oncol. 2022. PMID: 35216859
-
Worse Pituitary Adenoma Surgical Outcomes Predicted by Increasing Frailty, Not Age.World Neurosurg. 2022 May;161:e347-e354. doi: 10.1016/j.wneu.2022.02.002. Epub 2022 Feb 5. World Neurosurg. 2022. PMID: 35134588
-
Baseline frailty status, not advanced patient age, predicts epilepsy surgery outcomes: An analysis of 696 patients from the NSQIP database.Clin Neurol Neurosurg. 2023 Aug;231:107864. doi: 10.1016/j.clineuro.2023.107864. Epub 2023 Jun 26. Clin Neurol Neurosurg. 2023. PMID: 37390568
-
Frailty impact on postoperative complications and early mortality rates in patients undergoing radical cystectomy for bladder cancer: a systematic review.Arab J Urol. 2020 Nov 2;19(1):9-23. doi: 10.1080/2090598X.2020.1841538. Arab J Urol. 2020. PMID: 33763244 Free PMC article. Review.
Cited by
-
Integrated management of metastatic spinal tumors: current status and future directions.Med Oncol. 2025 May 14;42(6):210. doi: 10.1007/s12032-025-02764-8. Med Oncol. 2025. PMID: 40366495 Review.
-
Endoscopic and Nonendoscopic Approaches to Single-Level Lumbar Spine Decompression: Propensity Score-Matched Comparative Analysis and Frailty-Driven Predictive Model.Neurospine. 2023 Mar;20(1):119-128. doi: 10.14245/ns.2346110.055. Epub 2023 Mar 31. Neurospine. 2023. PMID: 37016860 Free PMC article.
-
Baseline Frailty Measured by the Risk Analysis Index and 30-Day Mortality After Surgery for Spinal Malignancy: Analysis of a Prospective Registry (2011-2020).Neurospine. 2024 Jun;21(2):404-413. doi: 10.14245/ns.2347120.560. Epub 2024 Jun 30. Neurospine. 2024. PMID: 38955517 Free PMC article.
-
The Fine Line Between Simplicity and Oversimplification: Comparing the Risk Analysis Index and 5-Factor Modified Frailty Index as Frailty Assessment Tools.Neurospine. 2023 Jun;20(2):728-730. doi: 10.14245/ns.2346496.248. Epub 2023 Jun 30. Neurospine. 2023. PMID: 37401092 Free PMC article. No abstract available.
-
The Risk Analysis Index Has Superior Discrimination Compared With the Modified Frailty Index-5 in Predicting Worse Postoperative Outcomes for the Octogenarian Neurosurgical Patient.Neurosurg Pract. 2023 Jun 15;4(3):e00044. doi: 10.1227/neuprac.0000000000000044. eCollection 2023 Sep. Neurosurg Pract. 2023. PMID: 39958794 Free PMC article.
References
-
- Mechtler LL, Nandigam K. Spinal cord tumors: new views and future directions. Neurol Clin. 2013;31:241–68. - PubMed
-
- Sharma M, Sonig A, Ambekar S, et al. Discharge dispositions, complications, and costs of hospitalization in spinal cord tumor surgery: analysis of data from the United States Nationwide Inpatient Sample, 2003-2010. Journal of neurosurgery. Spine. 2014;20:125–41. - PubMed
-
- Tihan T, Chi JH, McCormick PC, et al. Pathologic and epidemiologic findings of intramedullary spinal cord tumors. Neurosurg Clin N Am. 2006;17:7–11. - PubMed
-
- Kaloostian PE, Zadnik PL, Etame AB, et al. Surgical management of primary and metastatic spinal tumors. Cancer Control. 2014;21:133–9. - PubMed
LinkOut - more resources
Full Text Sources
