

Lifetime risk of cardiovascular-renal disease in type 2 diabetes: a population-based study in 473,399 individuals
- PMID: 35130878
- PMCID: PMC8822817
- DOI: 10.1186/s12916-022-02234-2
Lifetime risk of cardiovascular-renal disease in type 2 diabetes: a population-based study in 473,399 individuals
Erratum in
-
Correction to: Lifetime risk of cardiovascular-renal disease in type 2 diabetes: a population-based study in 473,399 individuals.BMC Med. 2022 Mar 23;20(1):121. doi: 10.1186/s12916-022-02308-1. BMC Med. 2022. PMID: 35317796 Free PMC article. No abstract available.
Abstract
Background: Cardiovascular and renal diseases (CVRD) are major causes of mortality in individuals with type 2 diabetes (T2D). Studies of lifetime risk have neither considered all CVRD together nor the relative contribution of major risk factors to combined disease burden.
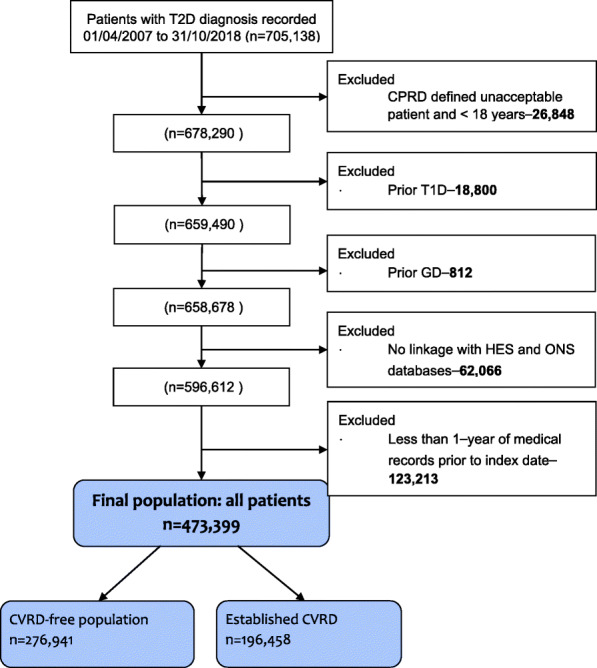
Methods: In a population-based cohort study using national electronic health records, we studied 473,399 individuals with T2D in England 2007-2018. Lifetime risk of individual and combined major adverse renal cardiovascular events, MARCE (including CV death and CVRD: heart failure; chronic kidney disease; myocardial infarction; stroke or peripheral artery disease), were estimated, accounting for baseline CVRD status and competing risk of death. We calculated population attributable risk for individual CVRD components. Ideal cardiovascular health was defined by blood pressure, cholesterol, glucose, smoking, physical activity, diet, and body mass index (i.e. modifiable risk factors).
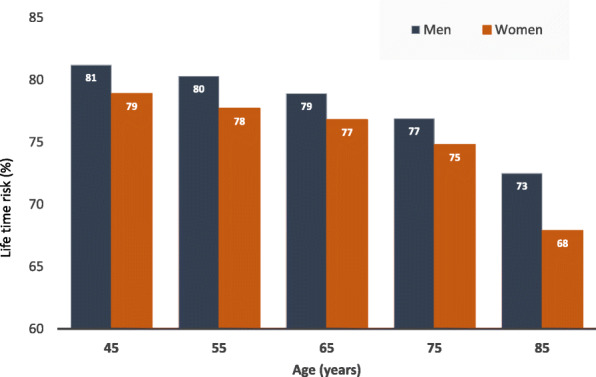
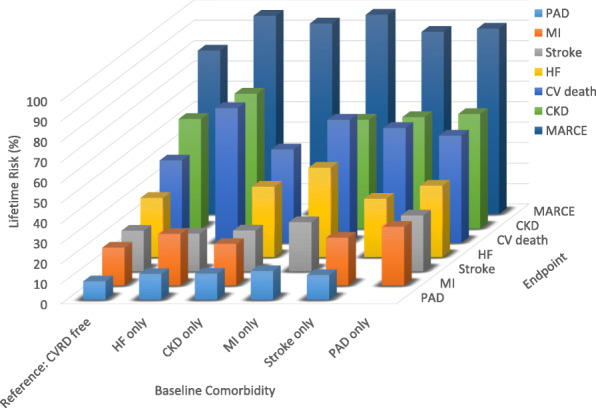
Results: In individuals with T2D, lifetime risk of MARCE was 80% in those free from CVRD and was 97%, 93%, 98%, 89% and 91% in individuals with heart failure, chronic kidney disease, myocardial infarction, stroke and peripheral arterial disease, respectively at baseline. Among CVRD-free individuals, lifetime risk of chronic kidney disease was highest (54%), followed by CV death (41%), heart failure (29%), stroke (20%), myocardial infarction (19%) and peripheral arterial disease (9%). In those with HF only, 75% of MARCE after index T2D can be attributed to HF after adjusting for age, gender, and comorbidities. Compared with those with > 1, < 3 and ≥3 modifiable health risk behaviours, achieving ideal cardiovascular health could reduce MARCE by approximately 41.5%, 23.6% and 17.2%, respectively, in the T2D population.
Conclusions: Four out of five individuals with T2D free from CVRD, and nearly all those with history of CVRD, will develop MARCE over their lifetime. Early preventive measures in T2D patients are clinical, public health and policy priorities.
Keywords: Attributable risk; Cardiovascular; Kidney; Lifetime; Population health; Type 2 diabetes.
© 2022. The Author(s).
Conflict of interest statement
AB is supported by research funding from NIHR, British Medical Association, AstraZeneca and UK Research and Innovation. HH is a National Institute for Health Research (NIHR) Senior Investigator. FA and HH are funded by the National Institute for Health Research University College London Hospitals Biomedical Research Centre. HH work is supported by: 1. Health Data Research UK (grant No. LOND1), which is funded by the UK Medical Research Council, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Department of Health and Social Care (England), Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Health and Social Care Research and Development Division (Welsh Government), Public Health Agency (Northern Ireland), British Heart Foundation and Wellcome Trust. AB, FA, SD and HH are part of the BigData@Heart Consortium, funded by the Innovative Medicines Initiative-2 Joint Undertaking under grant agreement No. 116074. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA; it is chaired, by DE Grobbee and SD Anker, partnering with 20 academic and industry partners and ESC. RZ, JBM, GG and TM are employed by AstraZeneca UK Ltd, a biopharmaceutical company.
Figures

References
-
- GBD 2017 Risk Factor Collaborators Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1923–1994. doi: 10.1016/S0140-6736(18)32225-6. - DOI - PMC - PubMed
-
- Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, Federici M, Filippatos G, Grobbee DE, Hansen TB, Huikuri HV, Johansson I, Jüni P, Lettino M, Marx N, Mellbin LG, Östgren CJ, Rocca B, Roffi M, Sattar N, Seferović PM, Sousa-Uva M, Valensi P, Wheeler DC. ESC Scientific Document Group. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41:255–323. doi: 10.1093/eurheartj/ehz486. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
