

The accuracy and robustness of plasma biomarker models for amyloid PET positivity
- PMID: 35130933
- PMCID: PMC8819863
- DOI: 10.1186/s13195-021-00942-0
The accuracy and robustness of plasma biomarker models for amyloid PET positivity
Abstract
Background: Plasma biomarkers for Alzheimer's disease (AD) have broad potential as screening tools in primary care and disease-modifying trials. Detecting elevated amyloid-β (Aβ) pathology to support trial recruitment or initiating Aβ-targeting treatments would be of critical value. In this study, we aimed to examine the robustness of plasma biomarkers to detect elevated Aβ pathology at different stages of the AD continuum. Beyond determining the best biomarker-or biomarker combination-for detecting this outcome, we also simulated increases in inter-assay coefficient of variability (CV) to account for external factors not considered by intra-assay variability. With this, we aimed to determine whether plasma biomarkers would maintain their accuracy if applied in a setting which anticipates higher variability (i.e., clinical routine).
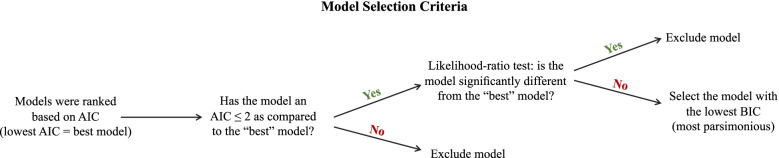
Methods: We included 118 participants (cognitively unimpaired [CU, n = 50], cognitively impaired [CI, n = 68]) from the ADNI study with a full plasma biomarker profile (Aβ42/40, GFAP, p-tau181, NfL) and matched amyloid imaging. Initially, we investigated how simulated CV variations impacted single-biomarker discriminative performance of amyloid status. Then, we evaluated the predictive performance of models containing different biomarker combinations, based both on original and simulated measurements. Plasma Aβ42/40 was represented by both immunoprecipitation mass spectrometry (IP-MS) and single molecule array (Simoa) methods in separate analyses. Model selection was based on a decision tree which incorporated Akaike information criterion value, likelihood ratio tests between the best-fitting models and, finally, and Schwartz's Bayesian information criterion.
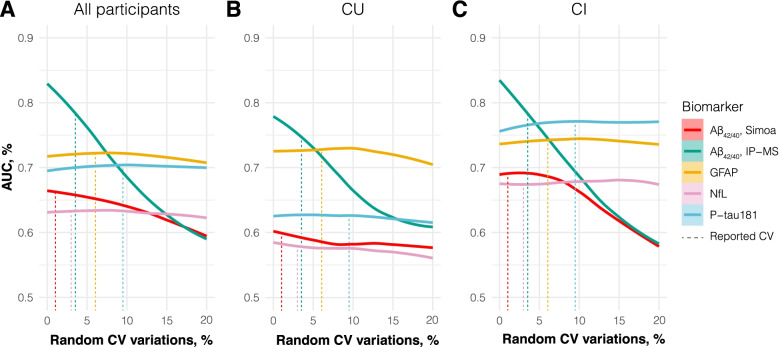
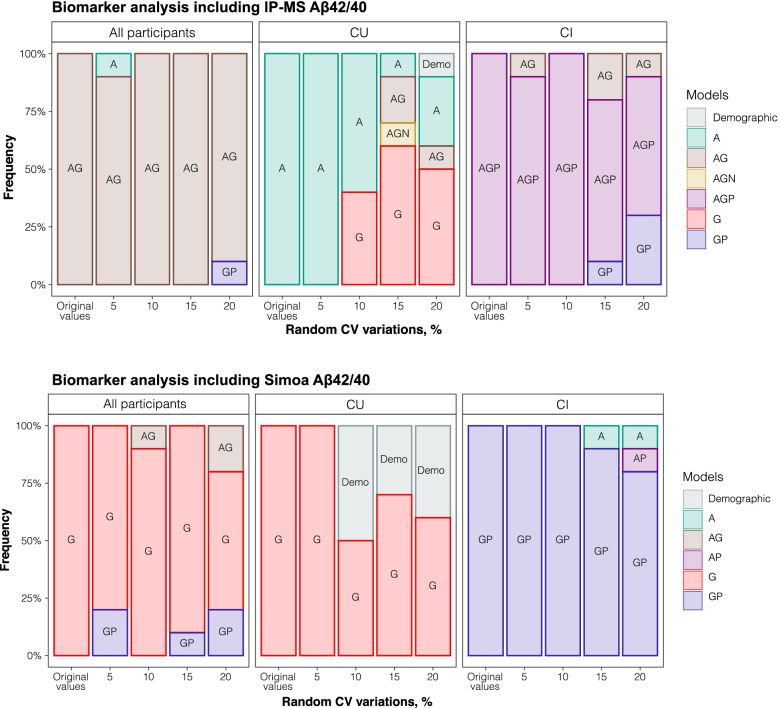
Results: Increasing variation greatly impacted the performance of plasma Aβ42/40 in discriminating Aβ status. In contrast, the performance of plasma GFAP and p-tau181 remained stable with variations >20%. When biomarker models were compared, the models "AG" (Aβ42/40 + GFAP; AUC = 86.5), "A" (Aβ42/40; AUC = 82.3), and "AGP" (Aβ42/40 + GFAP + p-tau181; AUC = 93.5) were superior in determining Aβ burden in all participants, within-CU, and within-CI groups, respectively. In the robustness analyses, when repeating model selection based on simulated measurements, models including IP-MS Aβ42/40 were also most often selected. Simoa Aβ42/40 did not contribute to any selected model when used as an immunoanalytical alternative to IP-MS Aβ42/40.
Conclusions: Plasma Aβ42/40, as quantified by IP-MS, shows high performance in determining Aβ positivity at all stages of the AD continuum, with GFAP and p-tau181 further contributing at CI stage. However, between-assay variations greatly impacted the performance of Aβ42/40 but not that of GFAP and p-tau181. Therefore, when dealing with between-assay CVs that exceed 5%, plasma GFAP and p-tau181 should be considered for a more robust determination of Aβ burden in CU and CI participants, respectively.
Keywords: ADNI; Alzheimer’s disease; Amyloid; GFAP; Immunoassay; Mass spectrometry; NfL; Plasma biomarker; p-tau181.
© 2022. The Author(s).
Conflict of interest statement
HZ has served at scientific advisory boards for Eisai, Denali, Roche Diagnostics, Wave, Samumed, Siemens Healthineers, Pinteon Therapeutics, Nervgen, AZTherapies, and CogRx, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure, and Biogen, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program. KB has served as a consultant, at advisory boards, or at data monitoring committees for Abcam, Axon, Biogen, JOMDD/Shimadzu. Julius Clinical, Lilly, MagQu, Novartis, Roche Diagnostics, and Siemens Healthineers, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program. OH has acquired research support (for the institution) from AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer, and Roche. In the past 2 years, he has received consultancy/speaker fees from Amylyx, Alzpath, Biogen, Cerveau, Fujirebio, Genentech, Roche, and Siemens.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
