

Detection of cerebral hypoperfusion with a dynamic hyperoxia test using brain oxygenation pressure monitoring
- PMID: 35130953
- PMCID: PMC8822803
- DOI: 10.1186/s13054-022-03918-0
Detection of cerebral hypoperfusion with a dynamic hyperoxia test using brain oxygenation pressure monitoring
Abstract
Introduction: Brain multimodal monitoring including intracranial pressure (ICP) and brain tissue oxygen pressure (PbtO2) is more accurate than ICP alone in detecting cerebral hypoperfusion after traumatic brain injury (TBI). No data are available for the predictive role of a dynamic hyperoxia test in brain-injured patients from diverse etiology.
Aim: To examine the accuracy of ICP, PbtO2 and the oxygen ratio (OxR) in detecting regional cerebral hypoperfusion, assessed using perfusion cerebral computed tomography (CTP) in patients with acute brain injury.
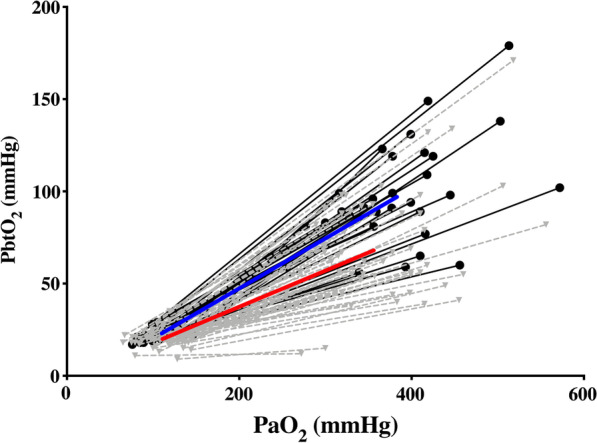
Methods: Single-center study including patients with TBI, subarachnoid hemorrhage (SAH) and intracranial hemorrhage (ICH) undergoing cerebral blood flow (CBF) measurements using CTP, concomitantly to ICP and PbtO2 monitoring. Before CTP, FiO2 was increased directly from baseline to 100% for a period of 20 min under stable conditions to test the PbtO2 catheter, as a standard of care. Cerebral monitoring data were recorded and samples were taken, allowing the measurement of arterial oxygen pressure (PaO2) and PbtO2 at FiO2 100% as well as calculation of OxR (= ΔPbtO2/ΔPaO2). Regional CBF (rCBF) was measured using CTP in the tissue area around intracranial monitoring by an independent radiologist, who was blind to the PbtO2 values. The accuracy of different monitoring tools to predict cerebral hypoperfusion (i.e., CBF < 35 mL/100 g × min) was assessed using area under the receiver-operating characteristic curves (AUCs).
Results: Eighty-seven CTPs were performed in 53 patients (median age 52 [41-63] years-TBI, n = 17; SAH, n = 29; ICH, n = 7). Cerebral hypoperfusion was observed in 56 (64%) CTPs: ICP, PbtO2 and OxR were significantly different between CTP with and without hypoperfusion. Also, rCBF was correlated with ICP (r = - 0.27; p = 0.01), PbtO2 (r = 0.36; p < 0.01) and OxR (r = 0.57; p < 0.01). Compared with ICP alone (AUC = 0.65 [95% CI, 0.53-0.76]), monitoring ICP + PbO2 (AUC = 0.78 [0.68-0.87]) or ICP + PbtO2 + OxR (AUC = 0.80 (0.70-0.91) was significantly more accurate in predicting cerebral hypoperfusion. The accuracy was not significantly different among different etiologies of brain injury.
Conclusions: The combination of ICP and PbtO2 monitoring provides a better detection of cerebral hypoperfusion than ICP alone in patients with acute brain injury. The use of dynamic hyperoxia test could not significantly increase the diagnostic accuracy.
Keywords: Brain injury; Hypoperfusion; Multimodal monitoring; Oxygen test.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Cooper DJ, Nichol AD, Bailey M, Bernard S, Cameron PA, Pili-Floury S, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR randomized clinical trial. JAMA. 2018;320(21):2211. doi: 10.1001/jama.2018.17075. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
