

Interruption of bile acid uptake by hepatocytes after acetaminophen overdose ameliorates hepatotoxicity
- PMID: 35131407
- PMCID: PMC9209783
- DOI: 10.1016/j.jhep.2022.01.020
Interruption of bile acid uptake by hepatocytes after acetaminophen overdose ameliorates hepatotoxicity
Abstract
Background & aims: Acetaminophen (APAP) overdose remains a frequent cause of acute liver failure, which is generally accompanied by increased levels of serum bile acids (BAs). However, the pathophysiological role of BAs remains elusive. Herein, we investigated the role of BAs in APAP-induced hepatotoxicity.
Methods: We performed intravital imaging to investigate BA transport in mice, quantified endogenous BA concentrations in the serum of mice and patients with APAP overdose, analyzed liver tissue and bile by mass spectrometry and MALDI-mass spectrometry imaging, assessed the integrity of the blood-bile barrier and the role of oxidative stress by immunostaining of tight junction proteins and intravital imaging of fluorescent markers, identified the intracellular cytotoxic concentrations of BAs, and performed interventions to block BA uptake from blood into hepatocytes.
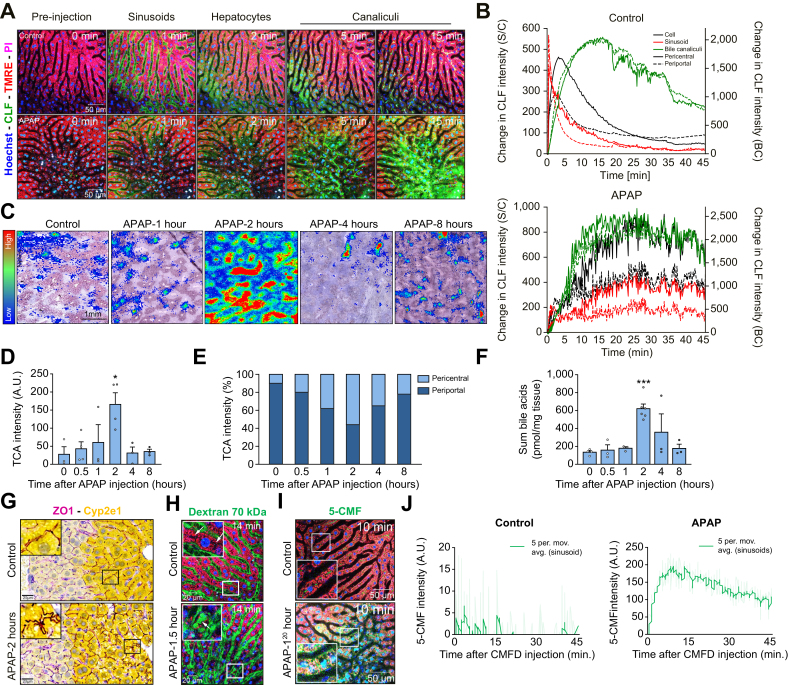
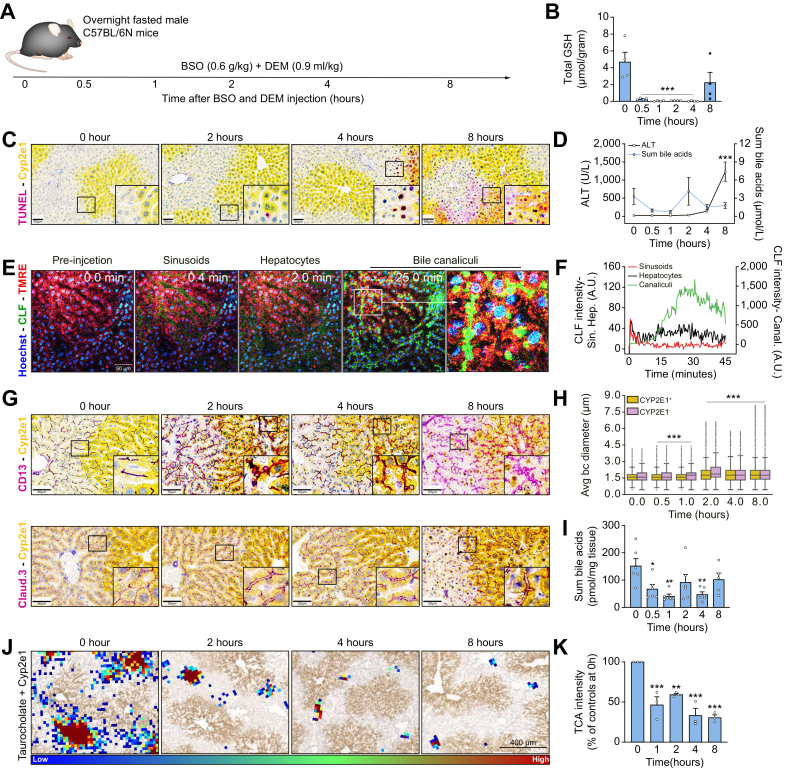
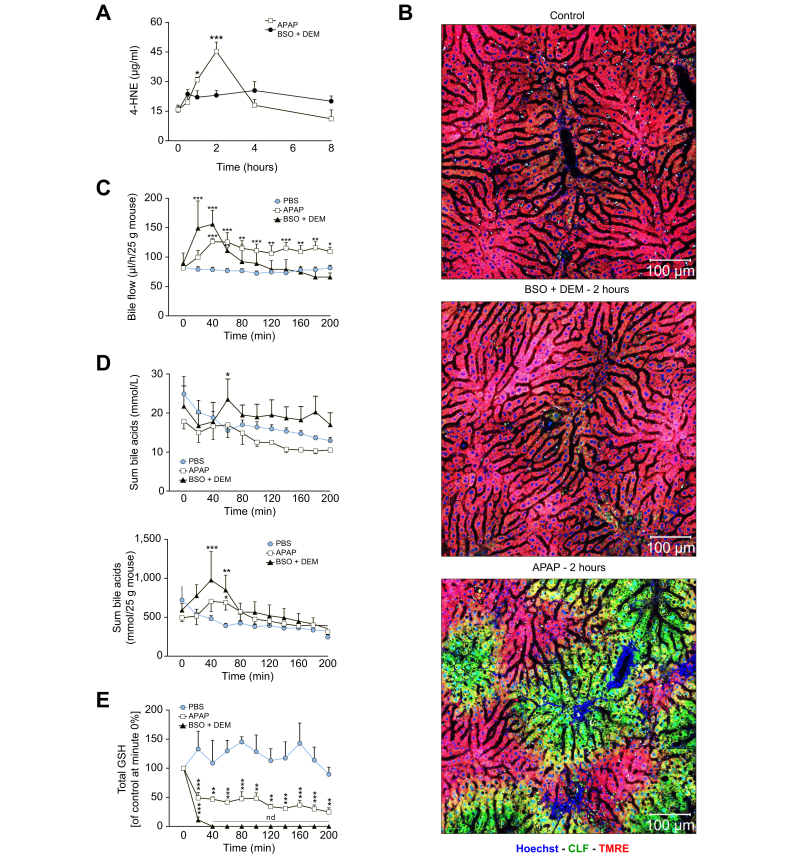
Results: Prior to the onset of cell death, APAP overdose causes massive oxidative stress in the pericentral lobular zone, which coincided with a breach of the blood-bile barrier. Consequently, BAs leak from the bile canaliculi into the sinusoidal blood, which is then followed by their uptake into hepatocytes via the basolateral membrane, their secretion into canaliculi and repeated cycling. This, what we termed 'futile cycling' of BAs, led to increased intracellular BA concentrations that were high enough to cause hepatocyte death. Importantly, however, the interruption of BA re-uptake by pharmacological NTCP blockage using Myrcludex B and Oatp knockout strongly reduced APAP-induced hepatotoxicity.
Conclusions: APAP overdose induces a breach of the blood-bile barrier which leads to futile BA cycling that causes hepatocyte death. Prevention of BA cycling may represent a therapeutic option after APAP intoxication.
Lay summary: Only one drug, N-acetylcysteine, is approved for the treatment of acetaminophen overdose and it is only effective when given within ∼8 hours after ingestion. We identified a mechanism by which acetaminophen overdose causes an increase in bile acid concentrations (to above toxic thresholds) in hepatocytes. Blocking this mechanism prevented acetaminophen-induced hepatotoxicity in mice and evidence from patients suggests that this therapy may be effective for longer periods after ingestion compared to N-acetylcysteine.
Keywords: APAP; acute liver failure; blood-bile barrier; intravital imaging; tight junctions.
Copyright © 2022 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest S.U. is holder and inventor on patents protecting Myrcludex B (Hepcludex/bulevirtide). All other authors declare that they have no conflict of interest. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures






References
-
- Bateman D.N. In: Critical Care Toxicology. Brent J., Burkhart K., Dargan P., Hatten B., Megarbane B., Palmer R., editors. Springer International Publishing; Cham: 2016. Acetaminophen (Paracetamol) pp. 1–25.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
