

Safety, patient acceptance and diagnostic accuracy of ultrasound core needle biopsy of parotid or submandibular glands in primary Sjögren's syndrome with suspected salivary gland lymphoma
- PMID: 35131750
- PMCID: PMC8823241
- DOI: 10.1136/rmdopen-2021-001901
Safety, patient acceptance and diagnostic accuracy of ultrasound core needle biopsy of parotid or submandibular glands in primary Sjögren's syndrome with suspected salivary gland lymphoma
Erratum in
-
Correction: Safety, patient acceptance and diagnostic accuracy of ultrasound core needle biopsy of parotid or submandibular glands in primary Sjögren's syndrome with suspected salivary gland lymphoma.RMD Open. 2022 Mar;8(1):e001901corr1. doi: 10.1136/rmdopen-2021-001901corr1. RMD Open. 2022. PMID: 35256535 Free PMC article. No abstract available.
Abstract
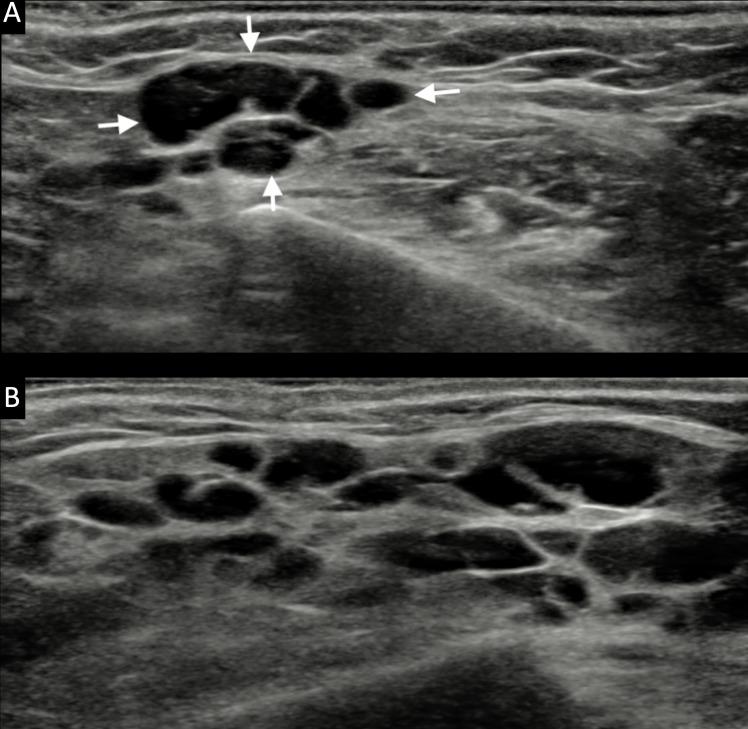
Background: Enlargement of the major salivary glands (SGs) is a major risk factor for B-cell lymphoma among patients with primary Sjögren's syndrome (pSS). Ultrasound-guided core needle biopsy (US-guided CNB) could be a novel technique to manage SG enlargement among patients with pSS.
Objective: Accordingly, this study's main aim was to evaluate the safety, patient tolerance and diagnostic accuracy of US-guided CNB procedure for patients with pSS with major SG enlargement.
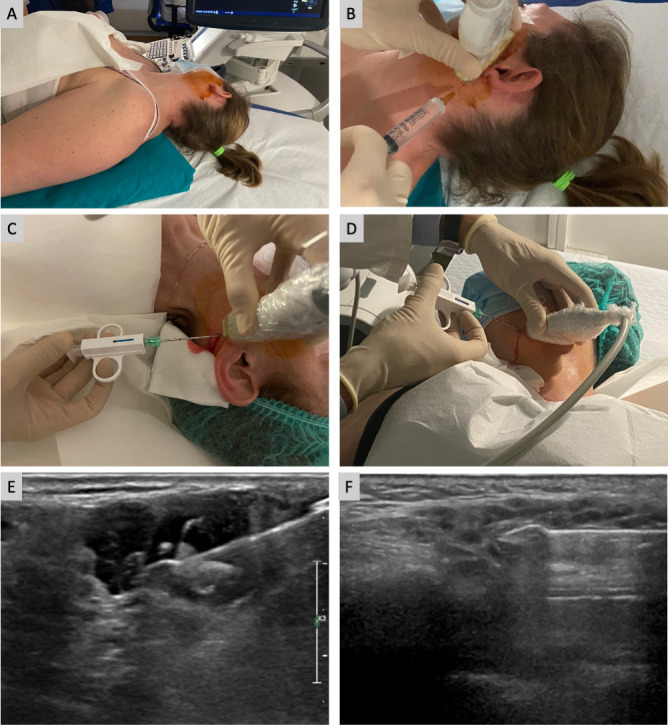
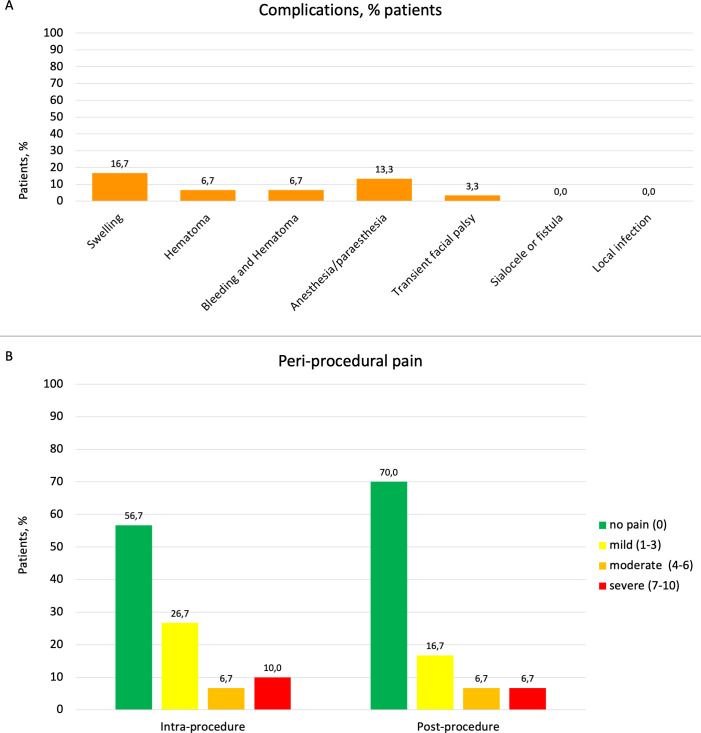
Methods: Patients with clinical diagnosis of pSS and a clinical indication for SG biopsy consecutively underwent US-guided CNB between September 2019 and June 2021. These patients were evaluated clinically 1, 2 and 12 weeks after US-guided CNB. Patients were asked to complete a questionnaire about postprocedural complications as well as periprocedural pain, using the Visual Analogue Scale. Complications were categorised as transient (<12 weeks) or persistent (≥12 weeks).
Results: US-guided CNB was performed on 30 major salivary glands (22 parotid glands and 8 submandibular glands). The procedure was well tolerated. Transient complications-such as haematoma, swelling-were observed among 43% of patients, and mean periprocedural pain was low. However, no persistent complications were reported during the study's follow-up period.
Conclusion: US-guided CNB represents a novel approach for the management of patients with pSS with SG enlargement. The procedure showed remarkable patient safety and tolerance, allowing adequate glandular sampling and a definite diagnosis for almost all participating patients without long-term complications.
Keywords: Sjogren's syndrome; autoimmune diseases; ultrasonography.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical