

Biological and Social Determinants of Hypertension Severity Before vs After Intracerebral Hemorrhage
- PMID: 35131909
- PMCID: PMC8967426
- DOI: 10.1212/WNL.0000000000200003
Biological and Social Determinants of Hypertension Severity Before vs After Intracerebral Hemorrhage
Abstract
Background and objectives: Although blood pressure (BP) control is considered the most effective measure to prevent functional decline after intracerebral hemorrhage (ICH), fewer than half of survivors achieve treatment goals. We hypothesized that long-term (i.e., prehemorrhage) hypertension severity may be a crucial factor in explaining poor BP control after ICH. We investigated changes in hypertension severity after vs before ICH using latent class analysis (LCA) and identified patient characteristics predictive of individuals' BP trajectories.
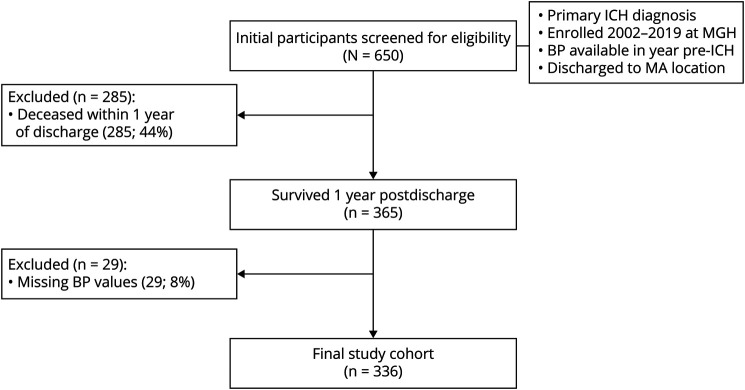
Methods: We analyzed data for ICH survivors enrolled in a study conducted at Massachusetts General Hospital (MGH) from 2002 to 2019 in Boston, a high-resource setting with near-universal medical insurance coverage. We captured BP measurements in the 12 months preceding and following the acute ICH hospitalization. Using LCA, we identified patient groups (classes) based on changes in hypertension severity over time in an unbiased manner. We then created multinomial logistic regression models to identify patient factors associated with these classes.
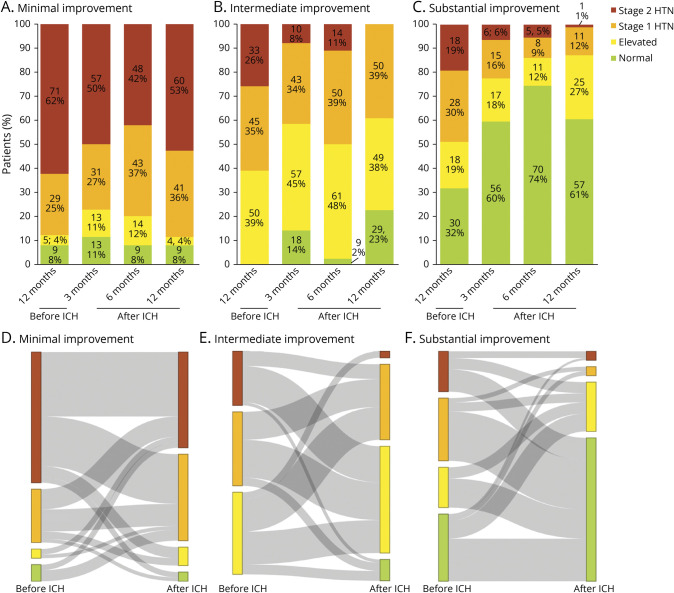
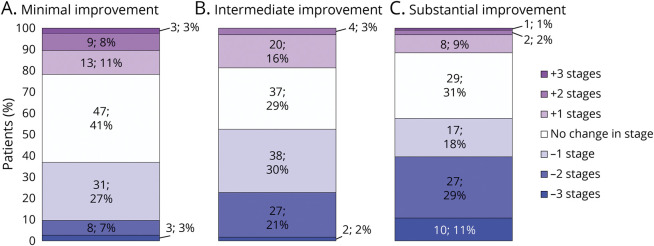
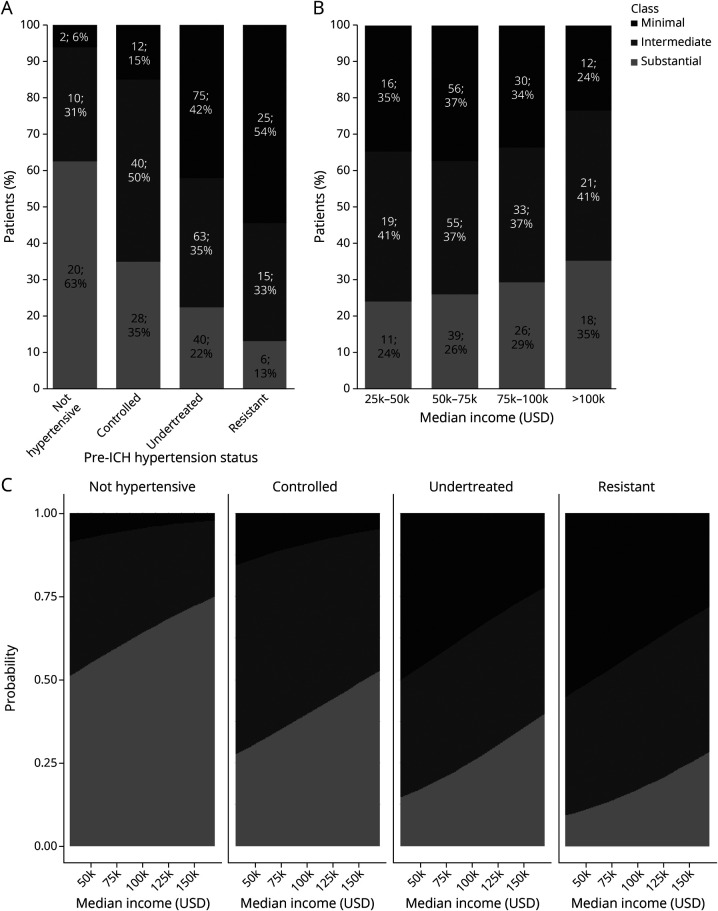
Results: Among 336 participants, the average age was 74.4 years, 166 (49%) were male, and 288 (86%) self-reported White race/ethnicity. LCA identified 3 patient classes, corresponding to minimal (n = 114, 34%), intermediate (n = 128, 38%), and substantial (n = 94, 28%) improvement in hypertension severity after vs before ICH. Survivors with undertreated (relative risk ratio [RRR] 0.05, 95% CI 0.01-0.23) or resistant (RRR 0.03, 95% CI 0.01-0.06) hypertension before ICH were less likely to experience substantial improvement afterwards. Residents of high-income neighborhoods were more likely to experience substantial improvement (RRR 1.14 per $10,000, 95% CI 1.02-1.28). Black, Hispanic, and Asian participants with uncontrolled hypertension before ICH were more likely to experience minimal improvement after hemorrhagic stroke (interaction p < 0.001).
Discussion: Most ICH survivors do not display consistent improvement in hypertension severity after hemorrhagic stroke. BP control after ICH is profoundly influenced by patient characteristics predating the hemorrhage, chiefly prestroke hypertension severity and socioeconomic status. Neighborhood income was associated with hypertension severity after ICH in a high-resource setting with near-universal health care coverage. These findings likely contribute to previously documented racial/ethnic disparities in BP control and clinical outcomes following ICH.
© 2022 American Academy of Neurology.
Figures
References
-
- Casolla B, Moulin S, Kyheng M, et al. Five-year risk of major ischemic and hemorrhagic events after intracerebral hemorrhage. Stroke. 2019;50:1100-1107. - PubMed
-
- Moulin S, Labreuche J, Bombois S, et al. Dementia risk after spontaneous intracerebral haemorrhage: a prospective cohort study. Lancet Neurol. 2016;15(8):820-829. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials