

Sleep health composites are associated with the risk of heart disease across sex and race
- PMID: 35132087
- PMCID: PMC8821698
- DOI: 10.1038/s41598-022-05203-0
Sleep health composites are associated with the risk of heart disease across sex and race
Abstract
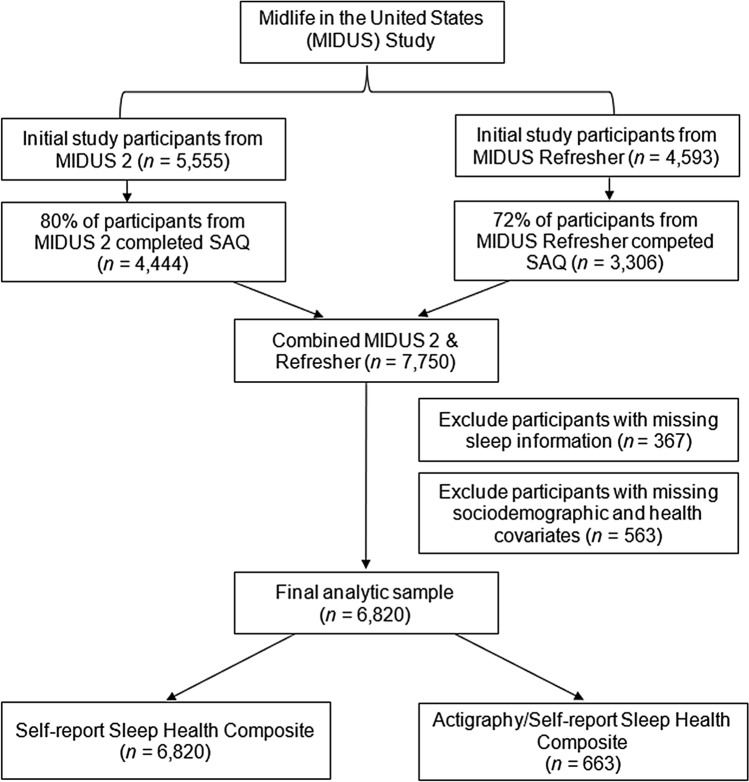
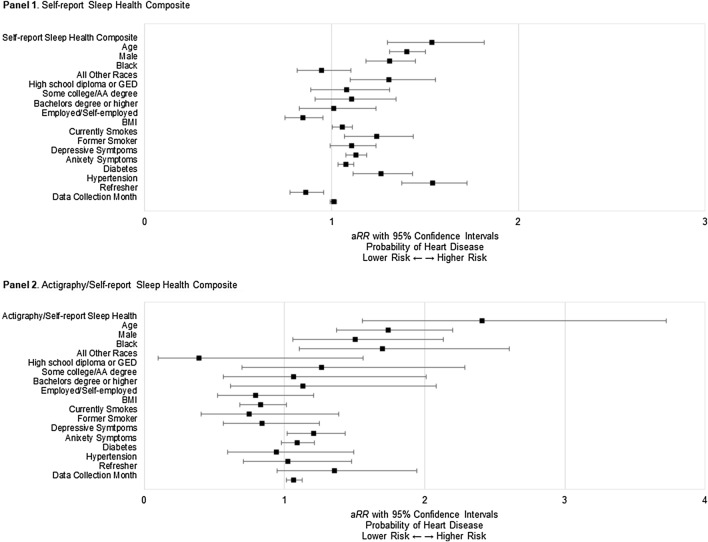
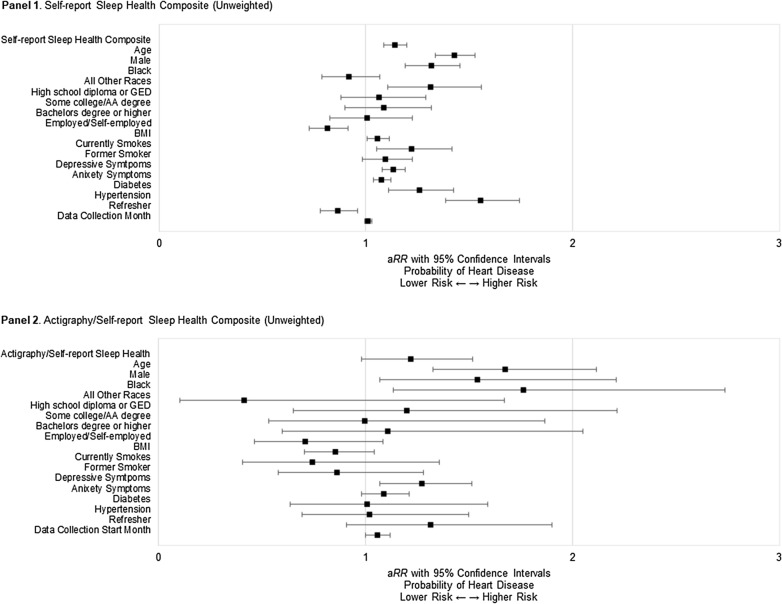
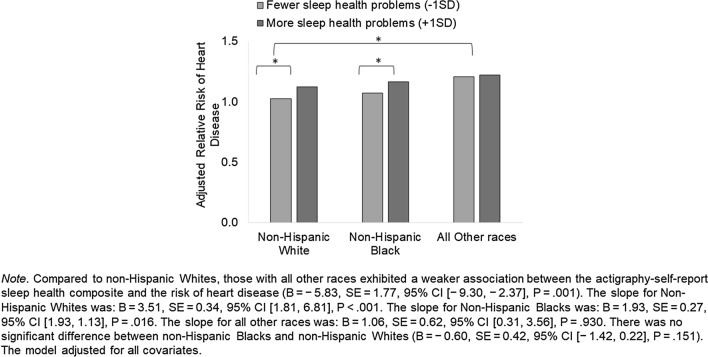
We examined whether subjectively and objectively measured sleep health composites have a relationship with heart disease. 6,820 adults (Mage = 53.4 years) from the Midlife in the United States study provided self-reported sleep characteristics and heart disease history. A smaller sample (n = 663) provided actigraphy sleep data. We tested two sleep health composites, based on self-report only and both self-report and actigraphy, across multiple sleep dimensions. We used a weighted sum approach, where higher scores indicated more sleep health problems. Modified Poisson regressions adjusted for sociodemographics and known risk factors. Having more sleep health problems was associated with a higher risk of heart disease using the self-report sleep health composite (aRR = 54%, P < .001) and the actigraphy/self-report composite (aRR = 141%, P < .001). Individual sleep dimensions of satisfaction, alertness, and efficiency (from the self-report composite) and regularity, satisfaction, and timing (from the actigraphy/self-report composite) were associated with the risk of heart disease. The effect size of each sleep health composite was larger than the individual sleep dimensions. Race moderated the association between the actigraphy/self-report sleep health composite and heart disease. There was no significant moderation by sex. Findings suggest poorer sleep health across multiple dimensions may contribute to heart disease risk among middle-aged adults.
© 2022. The Author(s).
Conflict of interest statement
All authors have no conflicts of interests related to the material presented. Soomi Lee discloses that she received a grant from NIH/National Institute on Aging (R56AG065251). Outside of the current work, O.M.B. received subcontract grants to Pennsylvania State University from Proactive Life (formerly Mobile Sleep Technologies) doing business as SleepSpace (National Science Foundation grant #1,622,766 and NIH/National Institute on Aging Small Business Innovation Research Program R43AG056250, R44 AG056250), honoraria/travel support for lectures from Boston University, Boston College, Tufts School of Dental Medicine, Harvard Chan School of Public Health, New York University, and Allstate®, consulting fees from Sleep Number, and an honorarium for his role as the Editor-in-Chief of Sleep Health (sleephealthjournal.org). Also outside the current work, M.L.W. provides statistical consulting for Noctem, Health Rhythms, and Sleep Number.
Figures
References
-
- Khan MS, Aouad R. The effects of insomnia and sleep loss on cardiovascular disease. Sleep Med. Clin. 2017;12:167–177. - PubMed
-
- Cappuccio FP, Cooper D, Delia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: A systematic review and meta-analysis of prospective studies. Eur. Heart J. 2011;32:1484–1492. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
