

Incidence trends for twelve cancers in younger adults-a rapid review
- PMID: 35132237
- PMCID: PMC9090760
- DOI: 10.1038/s41416-022-01704-x
Incidence trends for twelve cancers in younger adults-a rapid review
Abstract
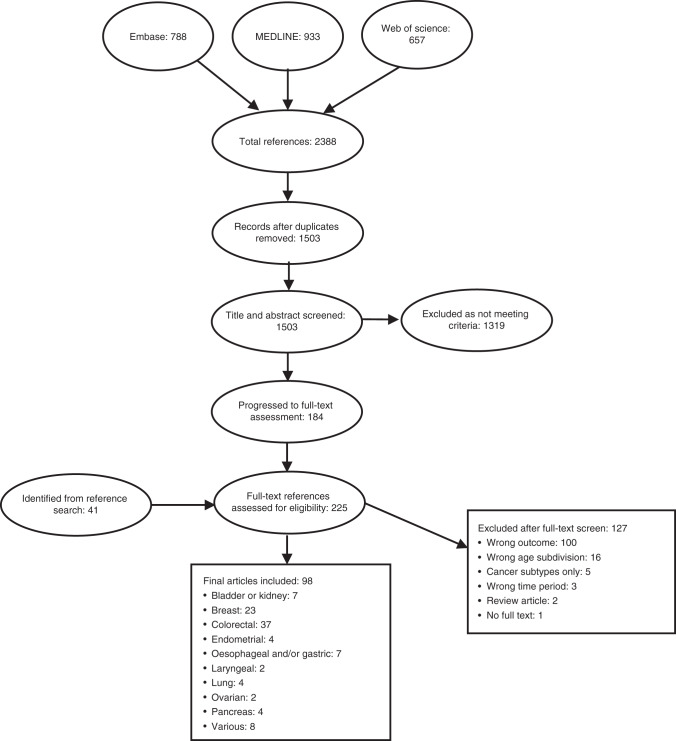
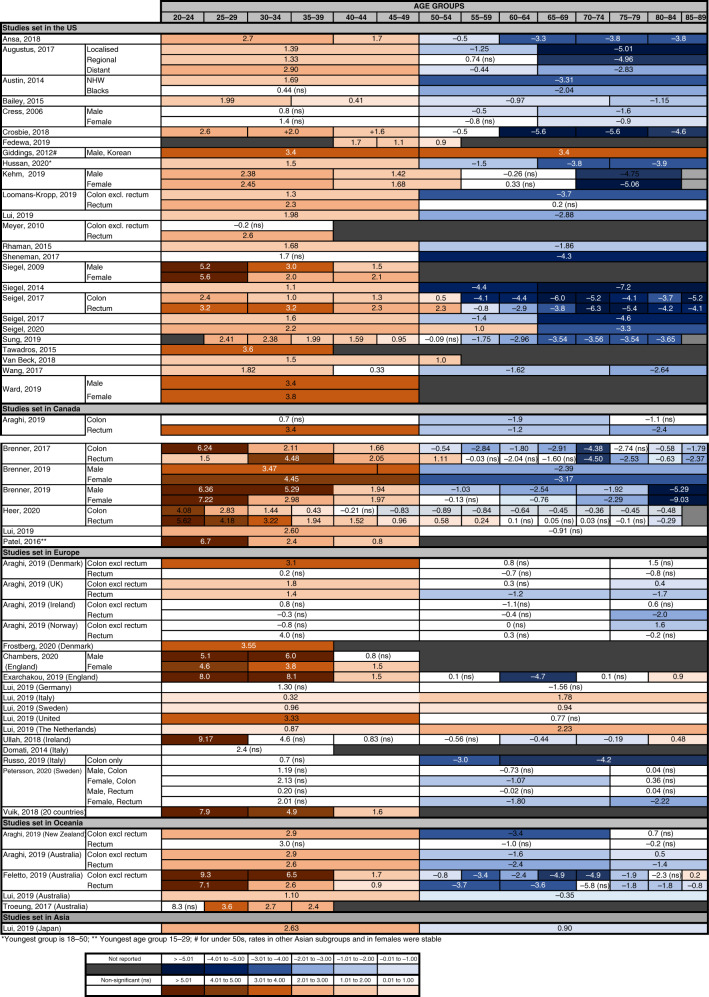
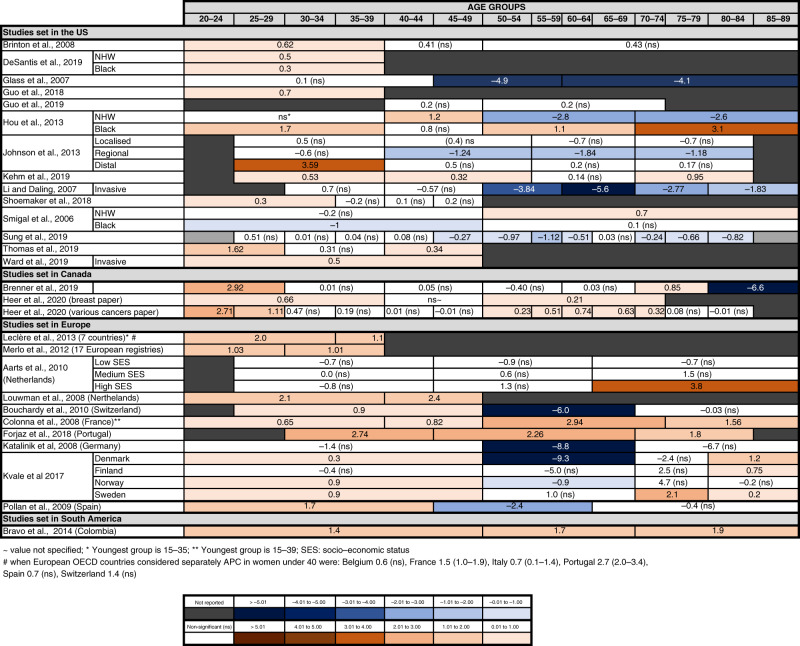
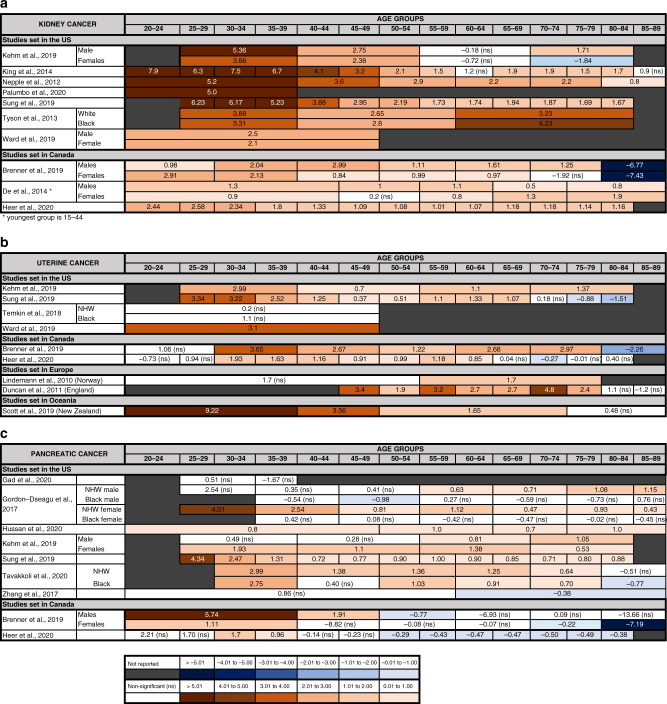
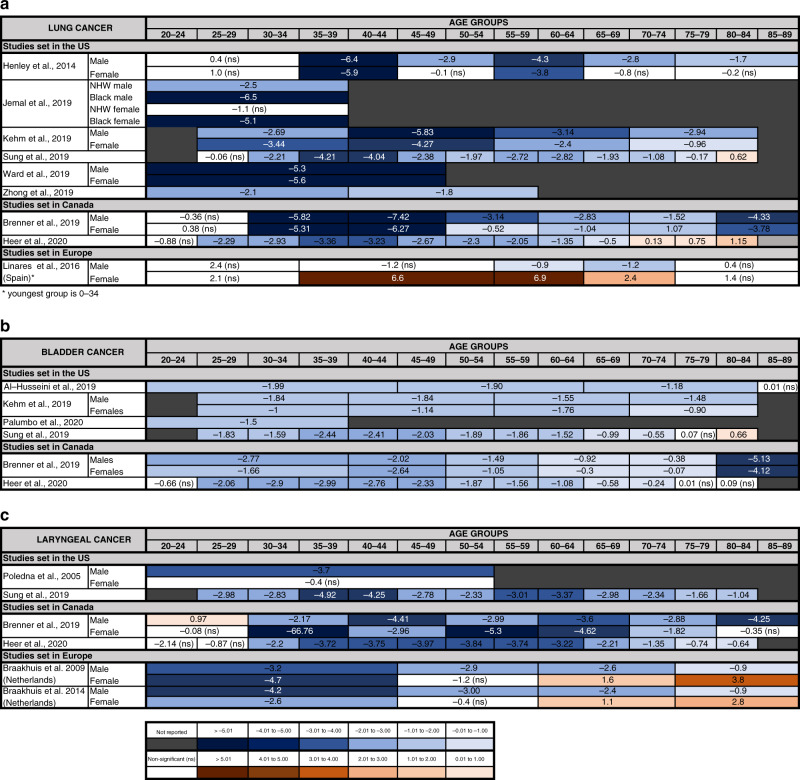
Many cancer referral guidelines use patient's age as a key criterium to decide who should be referred urgently. A recent rise in the incidence of colorectal cancer in younger adults has been described in high-income countries worldwide. Information on other cancers is more limited. The aim of this rapid review was to determine whether other cancers are also increasing in younger age groups, as this may have important implications for prioritising patients for investigation and referral. We searched MEDLINE, Embase and Web of Science for studies describing age-related incidence trends for colorectal, bladder, lung, oesophagus, pancreas, stomach, breast, ovarian, uterine, kidney and laryngeal cancer and myeloma. 'Younger' patients were defined based on NICE guidelines for cancer referral. Ninety-eight studies met the inclusion criteria. Findings show that the incidence of colorectal, breast, kidney, pancreas, uterine cancer is increasing in younger age groups, whilst the incidence of lung, laryngeal and bladder cancer is decreasing. Data for oesophageal, stomach, ovarian cancer and myeloma were inconclusive. Overall, this review provides evidence that some cancers are increasingly being diagnosed in younger age groups, although the mechanisms remain unclear. Cancer investigation and referral guidelines may need updating in light of these trends.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Lyratzopoulos G, Neal RD, Barbiere JM, Rubin GP, Abel GA. Variation in number of general practitioner consultations before hospital referral for cancer: findings from the 2010 National Cancer Patient Experience Survey in England. Lancet Oncol. 2012;13:353–65. doi: 10.1016/S1470-2045(12)70041-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
