

Giant Parathyroid Adenoma-Associated Fracture, Not All Lytic Bone Lesions are Cancer: A Case-Based Review
- PMID: 35132322
- PMCID: PMC8817849
- DOI: 10.1155/2022/3969542
Giant Parathyroid Adenoma-Associated Fracture, Not All Lytic Bone Lesions are Cancer: A Case-Based Review
Abstract
Introduction: Due to the early diagnosis of primary hyperparathyroidism the musculoskeletal manifestations of this disease are becoming less frequent. When this disease manifests secondary to a giant adenoma, it presents with more aggressive symptoms and can have important repercussions such as the hungry bone syndrome after parathyroidectomy. There are few reported cases of hyperparathyroidism secondary to a giant adenoma in the literature, as the presence of a brown tumor is often misinterpreted as a metastatic lesion from an unknown primary tumor.
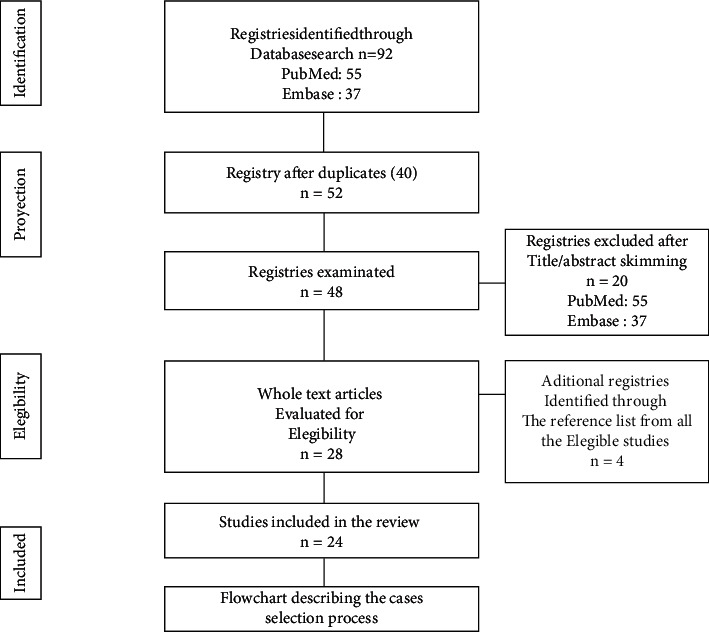
Methods: We describe a case and performed a literature review to identify all case reports. A literature search was carried out on PubMed/MEDLINE and EMBASE bibliographic databases. All available studies from May 2009 to May 2021 were included. Data were tabulated, and outcomes were cumulatively analyzed.
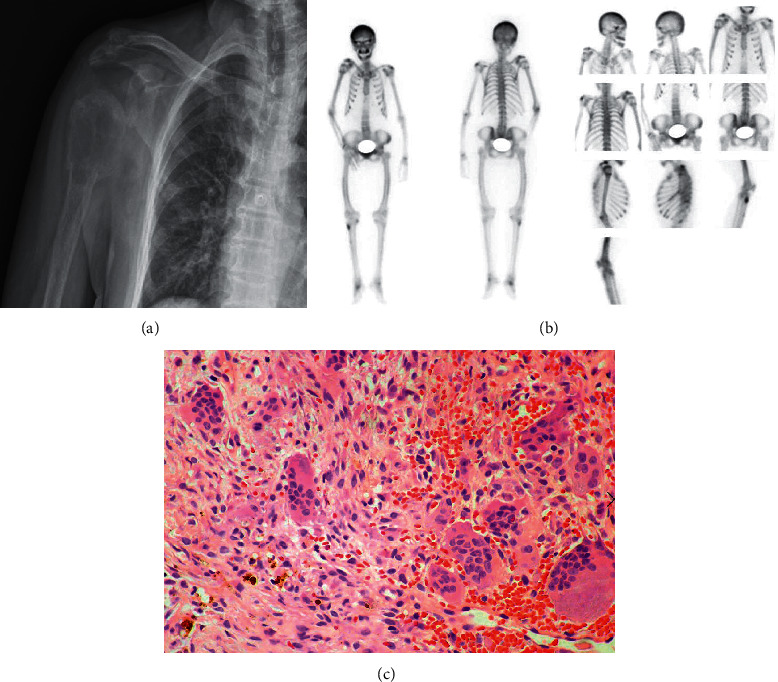
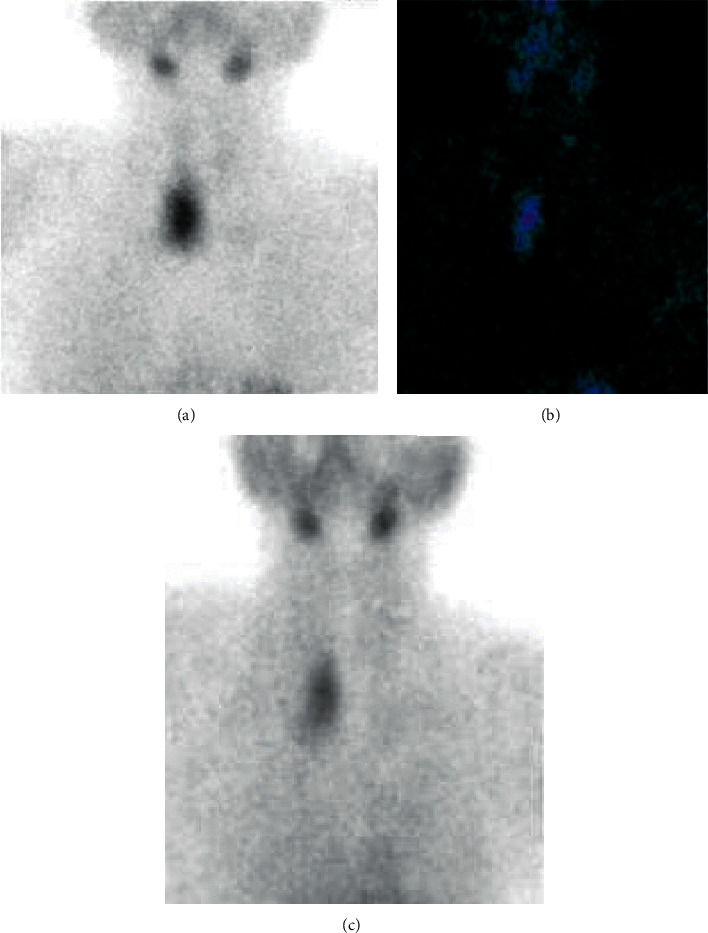
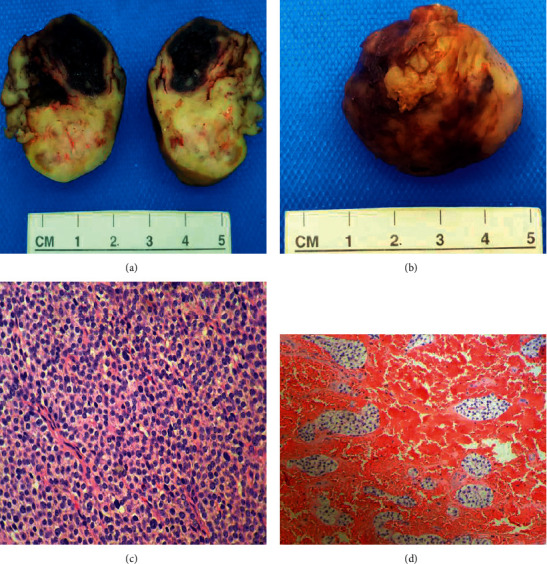
Results: Twenty-four cases of primary hyperparathyroidism due to giant adenoma have been described; the majority were women, with a mean age of 52 years. They presented with heterogeneous symptoms such as palpable nodules (45%), bone pain (33%), brown tumor (12.5%), asymptomatic (12.5%), metabolic profile with a mean calcemia of 13.8 mg/dL, PTH 1109 ng/L, and mean tumor weight of 47.24 g.
Conclusion: Primary hyperparathyroidism due to giant adenoma increases the risk of developing potentially serious postoperative complications such as hungry bone syndrome. This implies the need of implementing preventive measures comprising administration of intravenous zoledronic acid and early supplementation of oral calcium to prevent complications after resection.
Copyright © 2022 Jose C. Alvarez-Payares et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Giant Parathyroid Adenoma: A Case Report.Cureus. 2023 Jan 24;15(1):e34140. doi: 10.7759/cureus.34140. eCollection 2023 Jan. Cureus. 2023. PMID: 36843787 Free PMC article.
-
Giant parathyroid adenoma: a case report and review of the literature.J Med Case Rep. 2019 Nov 14;13(1):332. doi: 10.1186/s13256-019-2257-7. J Med Case Rep. 2019. PMID: 31722742 Free PMC article. Review.
-
Secondary hyperparathyroidism after removal of a parathyroid adenoma.Endocr Pract. 2002 Nov-Dec;8(6):429-32. doi: 10.4158/EP.8.6.429. Endocr Pract. 2002. PMID: 15260008
-
Giant parathyroid adenoma diagnosed by brown tumour, a clinical manifestation of primary hyperparathyroidism: A case report.J Pak Med Assoc. 2021 Apr;71(4):1266-1269. doi: 10.47391/JPMA.393. J Pak Med Assoc. 2021. PMID: 34125787
-
A Rare Case of Primary Hyperparathyroidism Caused by a Giant Solitary Parathyroid Adenoma.Am J Case Rep. 2018 Nov 8;19:1334-1337. doi: 10.12659/AJCR.911452. Am J Case Rep. 2018. PMID: 30405093 Free PMC article. Review.
Cited by
-
Brown Tumors: The Hidden Face of Primary and Renal Hyperparathyroidism Amid Real-Life Settings.J Clin Med. 2024 Jun 29;13(13):3847. doi: 10.3390/jcm13133847. J Clin Med. 2024. PMID: 38999413 Free PMC article.
-
Multiple fractures due to hungry bone syndrome following parathyroidectomy: a clinical case report and review of literature.Clin Diabetes Endocrinol. 2024 Aug 17;10(1):25. doi: 10.1186/s40842-024-00183-8. Clin Diabetes Endocrinol. 2024. PMID: 39152506 Free PMC article.
-
Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism.Diagnostics (Basel). 2023 Jun 2;13(11):1953. doi: 10.3390/diagnostics13111953. Diagnostics (Basel). 2023. PMID: 37296804 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
