

Systemic inflammatory syndrome in children with FARSA deficiency
- PMID: 35132614
- PMCID: PMC9303323
- DOI: 10.1111/cge.14120
Systemic inflammatory syndrome in children with FARSA deficiency
Abstract
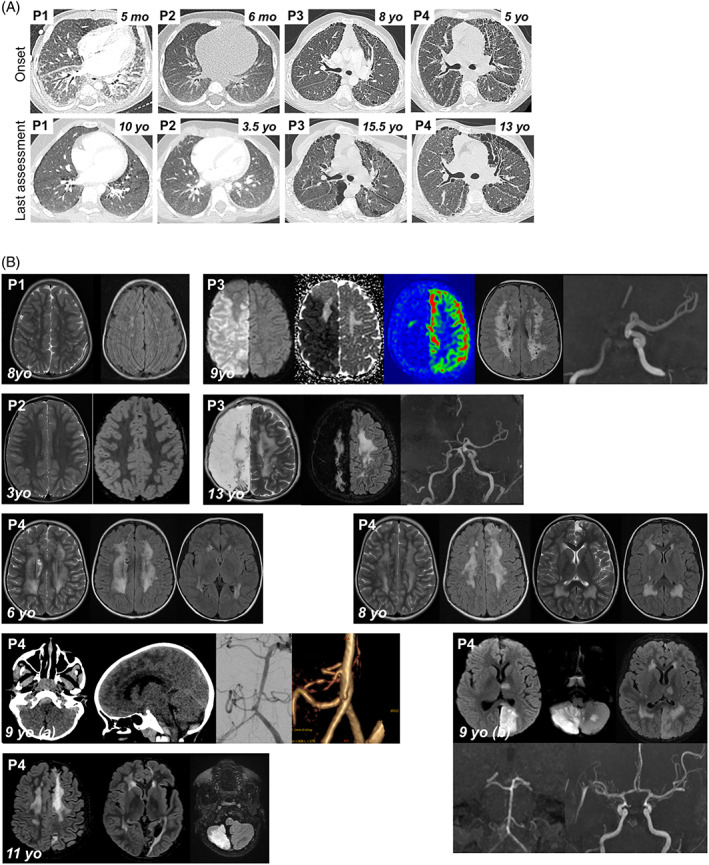
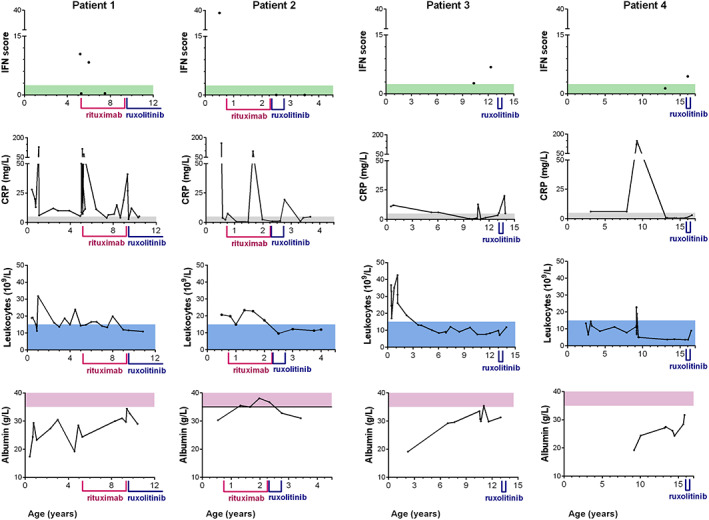
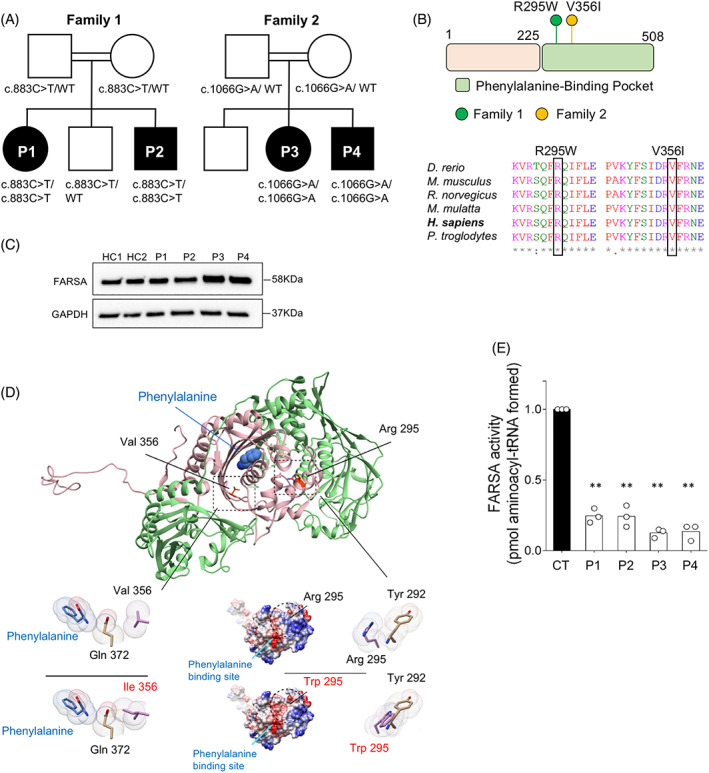
Variants in aminoacyl-tRNA synthetases (ARSs) genes are associated to a broad spectrum of human inherited diseases. Patients with defective PheRS, encoded by FARSA and FARSB, display brain abnormalities, interstitial lung disease and facial dysmorphism. We investigated four children from two unrelated consanguineous families carrying two missense homozygous variants in FARSA with significantly reduced PheRS-mediated aminoacylation activity. In addition to the core ARS-phenotype, all patients showed an inflammatory profile associated with autoimmunity and interferon score, a clinical feature not ascribed to PheRS-deficient patients to date. JAK inhibition improved lung disease in one patient. Our findings expand the genetic and clinical spectrum of FARSA-related disease.
Keywords: ARSopathy; FARSA; autoinflammation.
© 2022 The Authors. Clinical Genetics published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Antonellis A, Green ED. The role of aminoacyl‐tRNA synthetases in genetic diseases. Annu Rev Genom Hum Genet. 2008;9(1):87‐107. - PubMed
-
- Krenke K, Szczałuba K, Bielecka T, et al. FARSA mutations mimic phenylalanyl‐tRNA synthetase deficiency caused by FARSB defects. Clin Genet. 2019;96(5):468‐472. - PubMed
-
- Schuch LA, Forstner M, Rapp CK, et al. FARS1‐related disorders caused by bi‐allelic mutations in cytosolic phenylalanyl‐tRNA synthetase genes: look beyond the lungs! Clin Genet. 2021;99(6):789–801. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
