

Heart transplantation outcomes in arrhythmogenic right ventricular cardiomyopathy: a contemporary national analysis
- PMID: 35132806
- PMCID: PMC8934952
- DOI: 10.1002/ehf2.13687
Heart transplantation outcomes in arrhythmogenic right ventricular cardiomyopathy: a contemporary national analysis
Abstract
Aims: Heart failure is an increasingly recognized later stage manifestation of arrhythmogenic right ventricular cardiomyopathy (ARVC) that can require heart transplantation (HT) to appropriately treat. We aimed to study contemporary ARVC HT outcomes in a national registry.
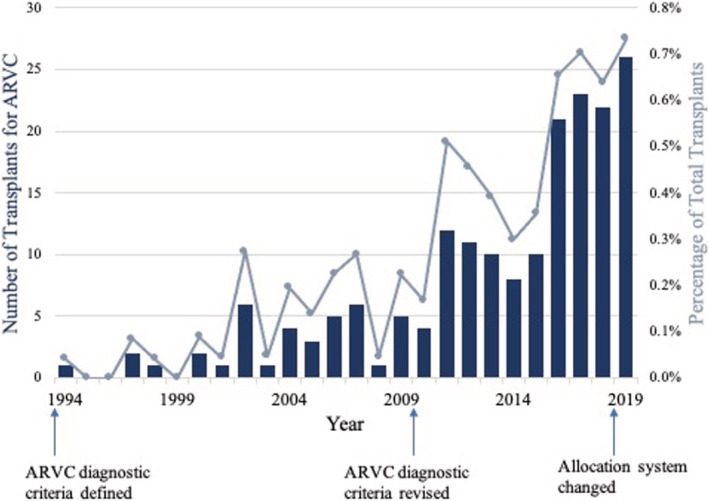
Methods and results: The United Network for Organ Sharing registry was queried for HT recipients from 1/1994 through 2/2020. ARVC patients were compared with non-ARVC dilated, restrictive, and hypertrophic cardiomyopathy HT patients (HT for ischaemic and valvular disease was excluded from analysis). Post-HT survival was assessed using Kaplan-Meier estimates. A total of 189 of 252 (75%) waitlisted ARVC patients (median age 48 years, 65% male) underwent HT, representing 0.3% of the total 65 559 HT during the study time period. Annual frequency of HT for ARVC increased significantly over time. ARVC patients had less diabetes (5% vs. 17%, P < 0.001), less cigarette use (15% vs. 23%, P < 0.001), lower pulmonary artery and pulmonary capillary wedge pressures, and lower cardiac output than the 33 659 non-ARVC patients (P < 0.001). Ventricular assist device use was significantly lower in ARVC patients (8% vs. 32%, P < 0.001); 1 and 5 year post-HT survival was 97% and 93% for ARVC vs. 95% and 82% for non-ARVC HT recipients (P < 0.001). On adjusted multivariable Cox regression, ARVC had decreased risk of post-HT death compared with non-ARVC aetiologies (hazard ratio 0.48, 95% confidence interval 0.28-0.82, P = 0.008). Patients with ARVC also had lower risk of death or graft failure than non-ARVC patients (hazard ratio 0.51, 95% confidence interval 0.32-0.81, P = 0.004).
Conclusions: In the largest series of HT in ARVC, we found that HT is increasingly performed in ARVC, with higher survival compared with other cardiomyopathy aetiologies. The right ventricular predominant pathophysiology may require unique considerations for heart failure management, including HT.
Keywords: Arrhythmogenic right ventricular cardiomyopathy; Heart failure; Heart transplantation; Post-transplant outcomes.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
H.T. is a consultant for Abbott. K.S. is a consultant and advisory board member and received honoraria from Novartis, Janssen, Bayer, Novo Nordisk, and Bristol Myers Squibb. H.C. is a consultant for Medtronic Inc., Biosense Webster, Pfizer, StrideBio, and Abbott. N.A.G. is a consultant and advisory board member for scPharmaceuticals, Inc. The remaining authors have no disclosures or possible conflicts of interest to report.
Figures


References
-
- Basso C, Corrado D, Marcus FI, Nava A, Thiene G. Arrhythmogenic right ventricular cardiomyopathy. The Lancet. 2009; 373: 1289‐1300. - PubMed
-
- Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, Calkins H, Corrado D, Cox MG, Daubert JP, Fontaine G, Gear K, Hauer R, Nava A, Picard MH, Protonotarios N, Saffitz JE, Sanborn DM, Steinberg JS, Tandri H, Thiene G, Towbin JA, Tsatsopoulou A, Wichter T, Zareba W. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the task force criteria. Circulation. 2010; 121: 1533‐1541. - PMC - PubMed
-
- Calkins H, Tandri H. Left Ventricular Involvement in ARVD/C. Circ Arrhythm Electrophysiol. 2015; 8: 1311‐1312. - PubMed
-
- Basso C, Thiene G, Corrado D, Angelini A, Nava A, Valente M. Arrhythmogenic right ventricular cardiomyopathy: Dysplasia, dystrophy, or myocarditis?. Circulation. 1996; 94: 983‐991. - PubMed
-
- Thiene G, Basso C. Arrhythmogenic right ventricular cardiomyopathy: An update. Cardiovasc Pathol. 2001; 10: 109‐117. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
