

Evaluating potential delays and outcomes of patients undergoing surgical resection for locally advanced and recurrent colorectal cancer during a pandemic
- PMID: 35132892
- PMCID: PMC9433197
- DOI: 10.1308/rcsann.2021.0274
Evaluating potential delays and outcomes of patients undergoing surgical resection for locally advanced and recurrent colorectal cancer during a pandemic
Abstract
Introduction: The COVID-19 pandemic resulted in a significant disruption of colorectal cancer (CRC) care pathways. This study evaluates the management and outcomes of patients with primary locally advanced or recurrent CRC during the pandemic in a single tertiary referral centre.
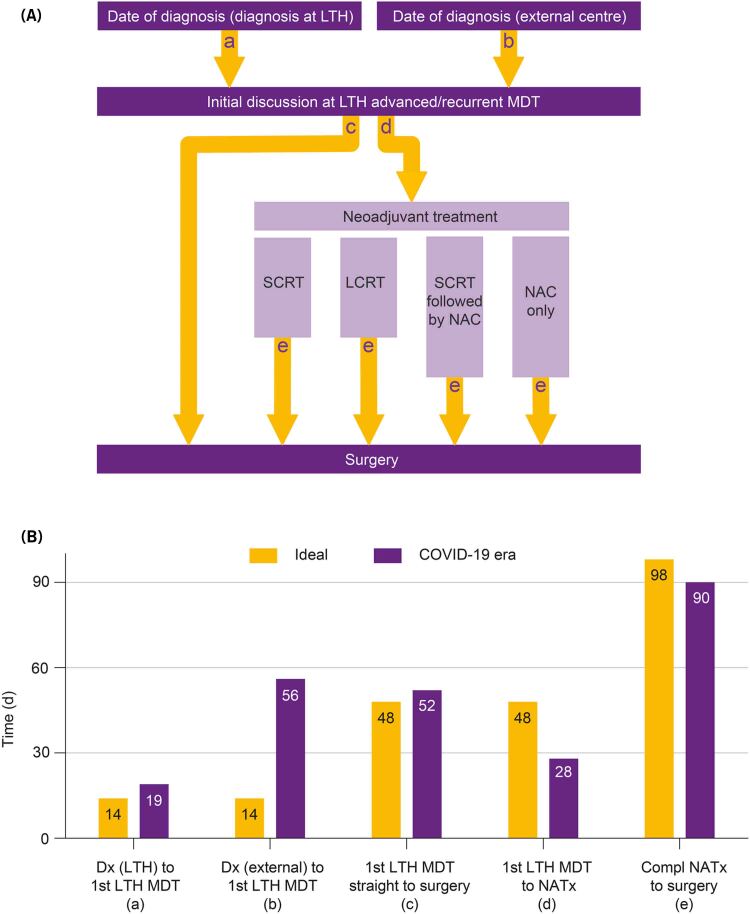
Methods: Patients undergoing elective surgery for advanced or recurrent CRC with curative intent between March 2020 and March 2021 were identified. Following first multidisciplinary team discussion patients were broadly classified into two groups: straight to surgery (n=22, 45%) or neoadjuvant therapy followed by surgery (n=27, 55%). Primary outcome was COVID-19-related complication rate.
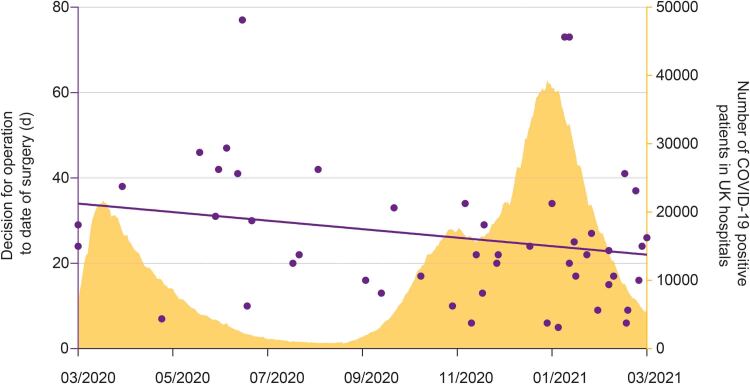
Results: Forty-nine patients with a median age of 66 years (interquartile range: 54-73) were included. No patients developed a COVID-19 infection or related complication during hospital admission. Significant delays were identified in the treatment pathway of patients in the straight to surgery group, mostly due to delays in referral from external centres. Nine of 22 patients in the straight to surgery group had evidence of tumour progression compared with 3 of 27 in the neoadjuvant group (p=0.015839). Seven of 27 patients in the neoadjuvant group showed evidence of tumour regression. During the study, surgical waiting times were reduced, and more operations were performed during the second wave of COVID-19.
Conclusion: This study suggests that it is possible to mitigate the risks of COVID-19-related complications in patients undergoing complex surgery for locally advanced and recurrent CRC. Delay in surgical intervention is associated with tumour progression, particularly in patients who may not have neoadjuvant therapy. Efforts should be made to prioritise resources for patients requiring time-sensitive surgery for advanced and recurrent CRC.
Keywords: Advanced colorectal cancer; COVID-19; Recurrent colorectal cancer; Surgery.
Figures

Similar articles
-
The impact of the Covid 19 pandemic in colorectal cancer.Ann Ital Chir. 2023;94:322-328. Ann Ital Chir. 2023. PMID: 37530050
-
Surgery for locally advanced recurrent colorectal cancer involving the aortoiliac axis: can we achieve R0 resection and long-term survival?Dis Colon Rectum. 2013 Jun;56(6):711-6. doi: 10.1097/DCR.0b013e31827dbcb0. Dis Colon Rectum. 2013. PMID: 23652744
-
Surgical approach in locally advanced colorectal cancer--combined, extended and compound surgery.Khirurgiia (Sofiia). 2013;(4):29-50. Khirurgiia (Sofiia). 2013. PMID: 24800318 Review. Bulgarian, English.
-
Neoadjuvant PD-1 blockade with toripalimab, with or without celecoxib, in mismatch repair-deficient or microsatellite instability-high, locally advanced, colorectal cancer (PICC): a single-centre, parallel-group, non-comparative, randomised, phase 2 trial.Lancet Gastroenterol Hepatol. 2022 Jan;7(1):38-48. doi: 10.1016/S2468-1253(21)00348-4. Epub 2021 Oct 22. Lancet Gastroenterol Hepatol. 2022. PMID: 34688374 Clinical Trial.
-
Clinical review: surgical management of locally advanced and recurrent colorectal cancer.Langenbecks Arch Surg. 2014 Jan;399(1):33-40. doi: 10.1007/s00423-013-1134-x. Epub 2013 Nov 19. Langenbecks Arch Surg. 2014. PMID: 24249035 Review.
Cited by
-
Open versus robotic-assisted techniques for multivisceral pelvic resections of locally advanced or recurrent colorectal and anal cancers: short-term outcomes from a single centre.Tech Coloproctol. 2024 Nov 19;28(1):161. doi: 10.1007/s10151-024-03044-9. Tech Coloproctol. 2024. PMID: 39560793 Free PMC article.
-
Global elective breast- and colorectal cancer surgery performance backlogs, attributable mortality and implemented health system responses during the COVID-19 pandemic: A scoping review.PLOS Glob Public Health. 2023 Apr 4;3(4):e0001413. doi: 10.1371/journal.pgph.0001413. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37014874 Free PMC article.
References
-
- Beyond TMEC. Consensus statement on the multidisciplinary management of patients with recurrent and primary rectal cancer beyond total mesorectal excision planes. Br J Surg 2013; 100: E1–E33. - PubMed
-
- Palmer G, Martling A, Cedermark B, Holm T. A population-based study on the management and outcome in patients with locally recurrent rectal cancer. Ann Surg Oncol 2007; 14: 447–454. - PubMed
-
- PelvEx C. Surgical and survival outcomes following pelvic exenteration for locally advanced primary rectal cancer: results from an international collaboration. Ann Surg 2019; 269: 315–321. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical