High-resolution structure-function mapping of intact hearts reveals altered sympathetic control of infarct border zones
- PMID: 35132963
- PMCID: PMC8855798
- DOI: 10.1172/jci.insight.153913
High-resolution structure-function mapping of intact hearts reveals altered sympathetic control of infarct border zones
Abstract
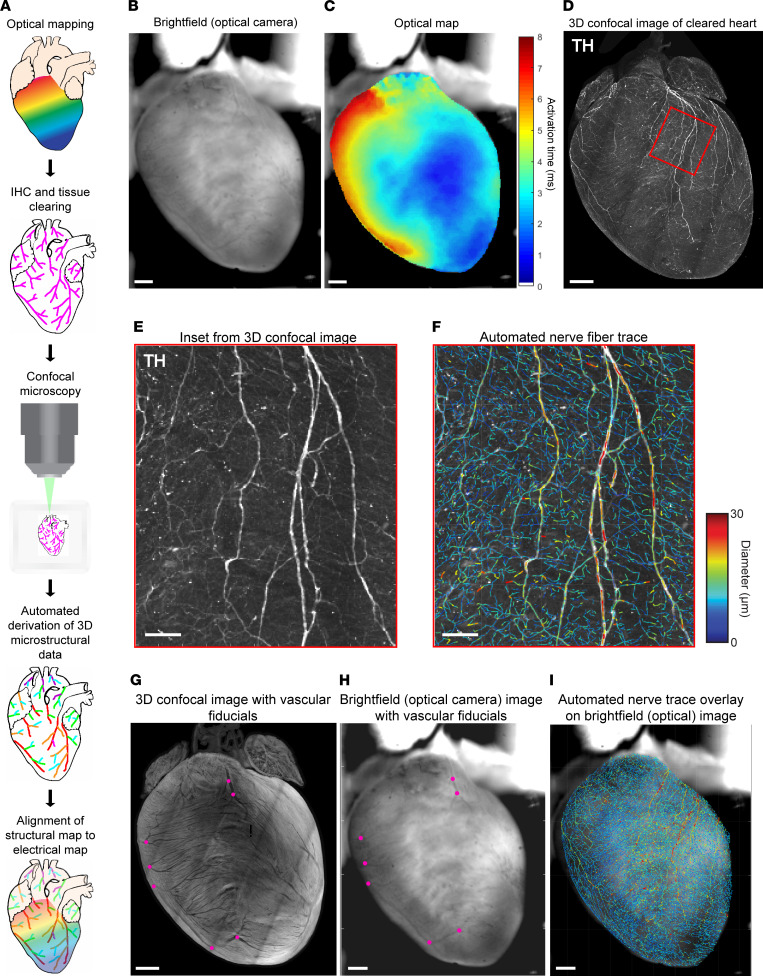
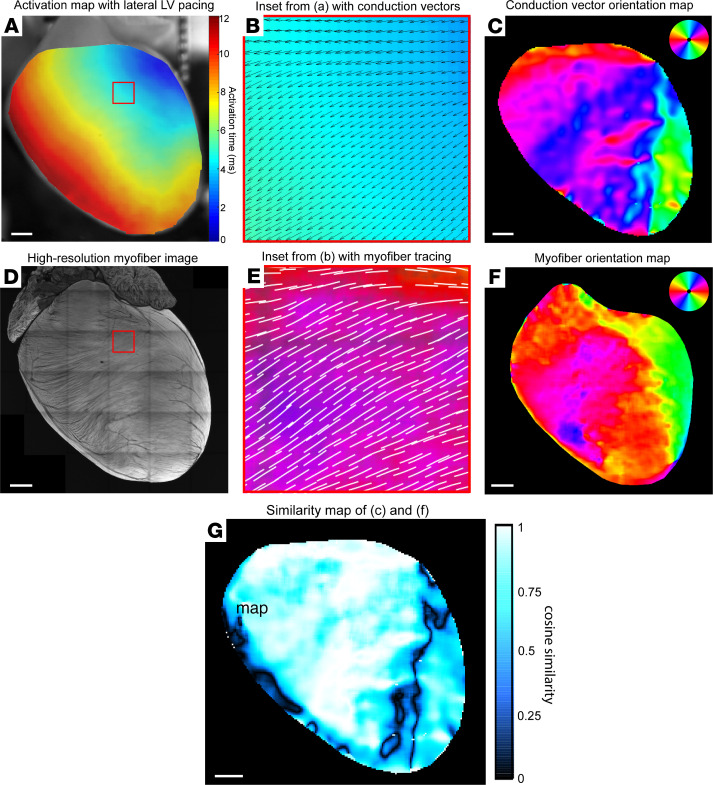
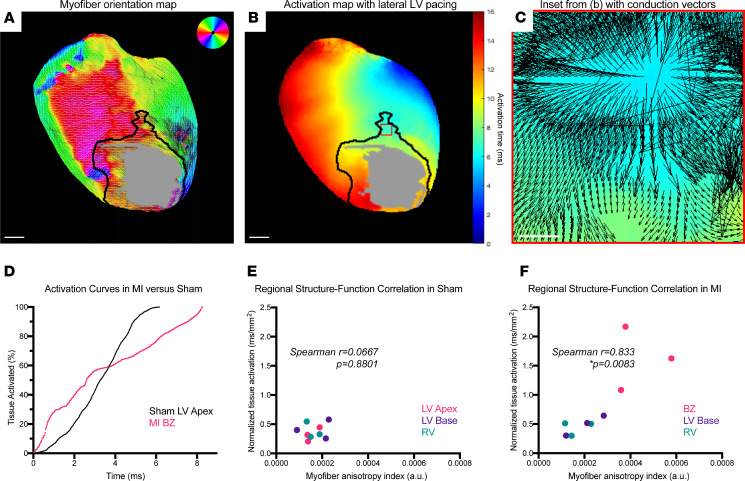
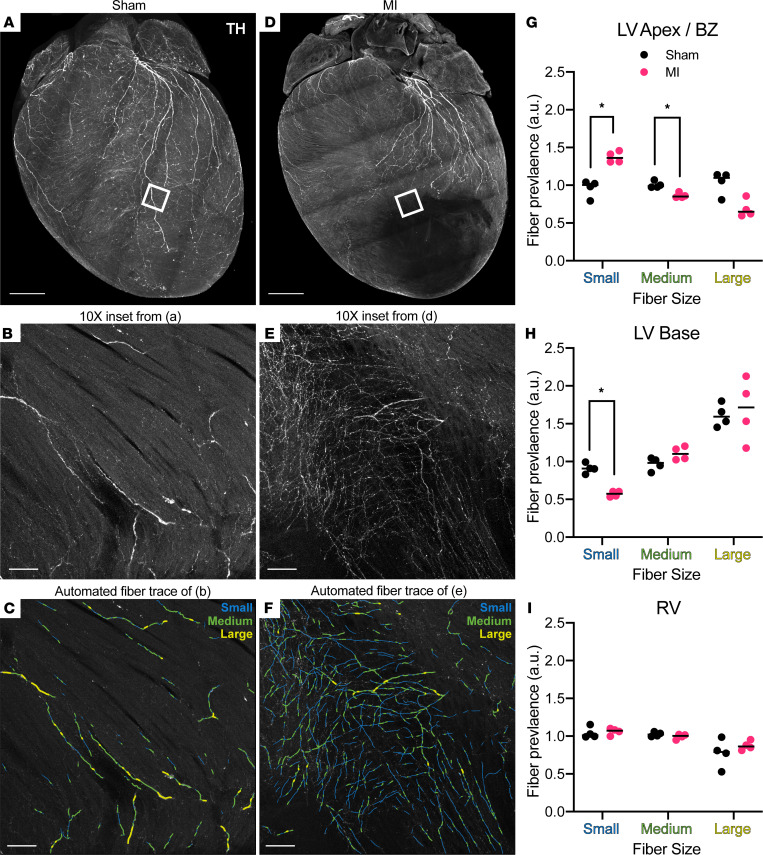
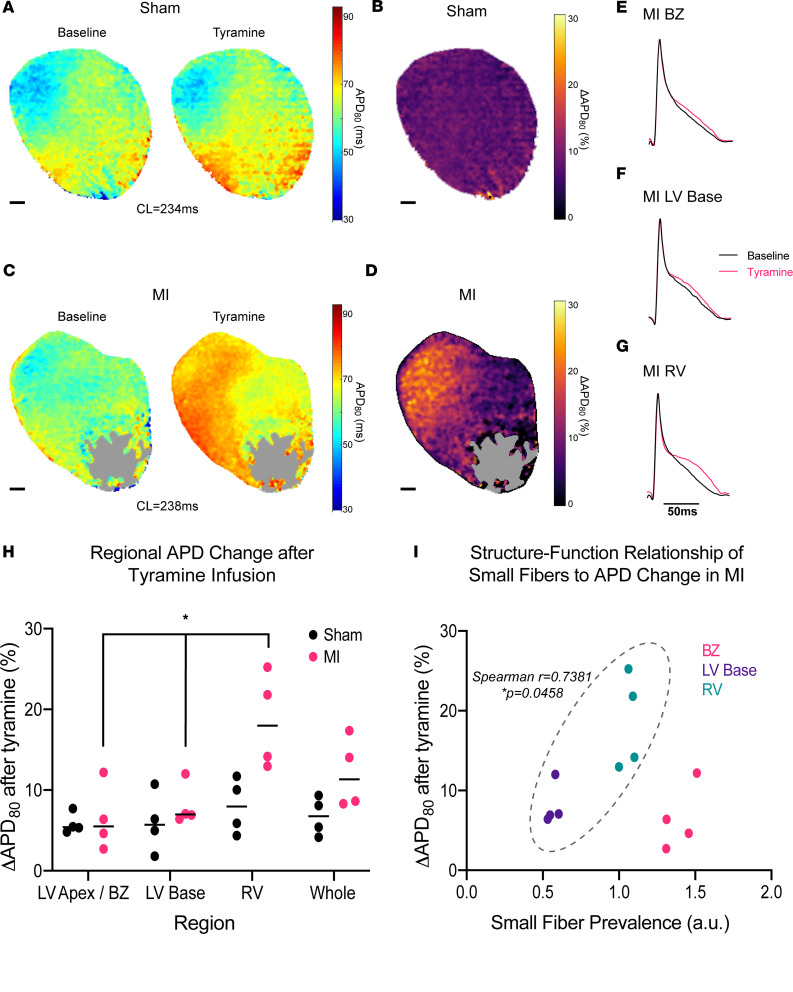
Remodeling of injured sympathetic nerves on the heart after myocardial infarction (MI) contributes to adverse outcomes such as sudden arrhythmic death, yet the underlying structural mechanisms are poorly understood. We sought to examine microstructural changes on the heart after MI and to directly link these changes with electrical dysfunction. We developed a high-resolution pipeline for anatomically precise alignment of electrical maps with structural myofiber and nerve-fiber maps created by customized computer vision algorithms. Using this integrative approach in a mouse model, we identified distinct structure-function correlates to objectively delineate the infarct border zone, a known source of arrhythmias after MI. During tyramine-induced sympathetic nerve activation, we demonstrated regional patterns of altered electrical conduction aligned directly with altered neuroeffector junction distribution, pointing to potential neural substrates for cardiac arrhythmia. This study establishes a synergistic framework for examining structure-function relationships after MI with microscopic precision that has potential to advance understanding of arrhythmogenic mechanisms.
Keywords: Arrhythmias; Cardiology; Innervation; Mouse models.
Conflict of interest statement
Figures