

Epilepsy and Pregnancy
- PMID: 35133310
- PMCID: PMC9642109
- DOI: 10.1212/CON.0000000000001056
Epilepsy and Pregnancy
Abstract
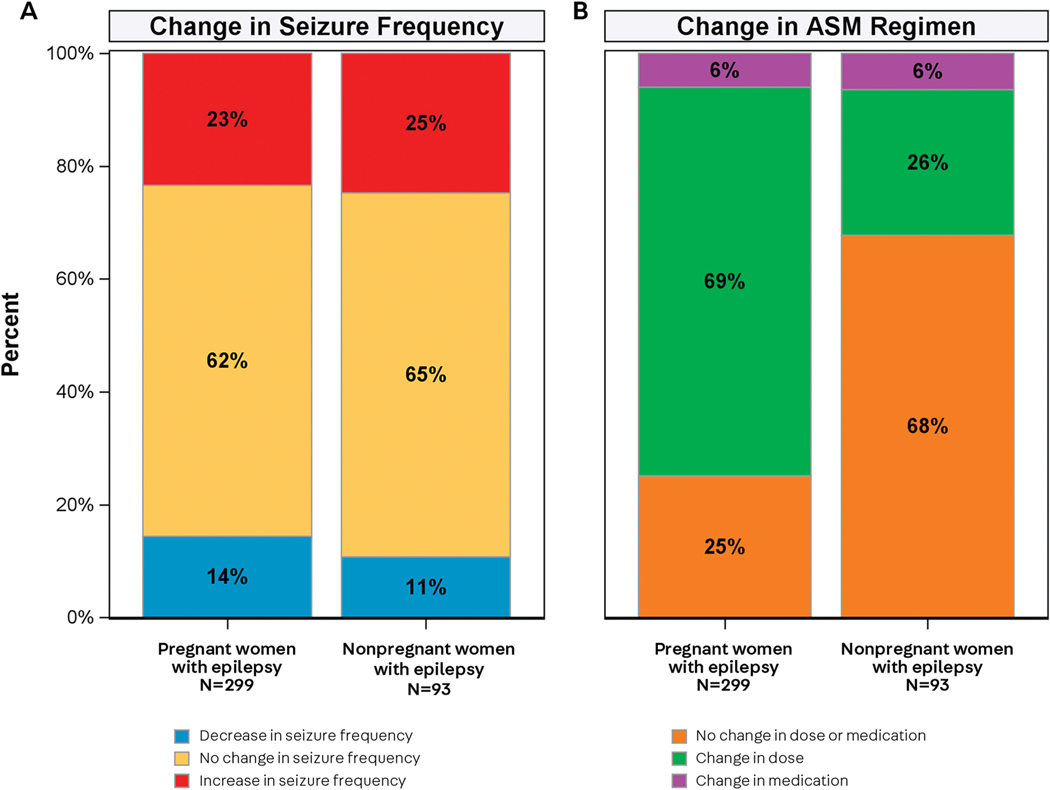
Purpose of review: Seizure disorders are the most frequent major neurologic complication in pregnancy, affecting 0.3% to 0.8% of all gestations. Women of childbearing age with epilepsy require special care related to pregnancy. This article provides up-to-date information to guide practitioners in the management of epilepsy in pregnancy.
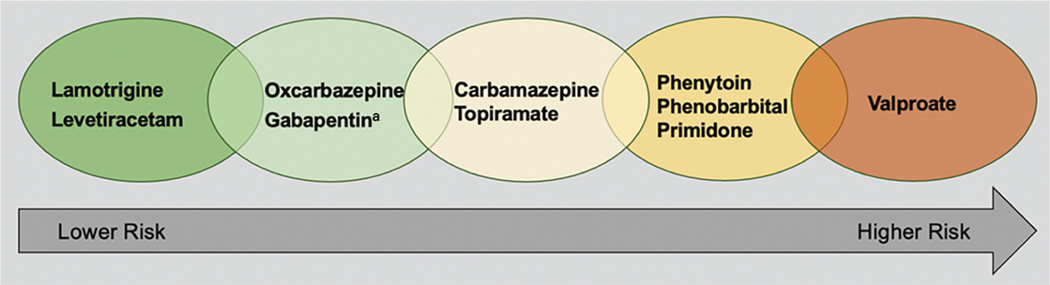
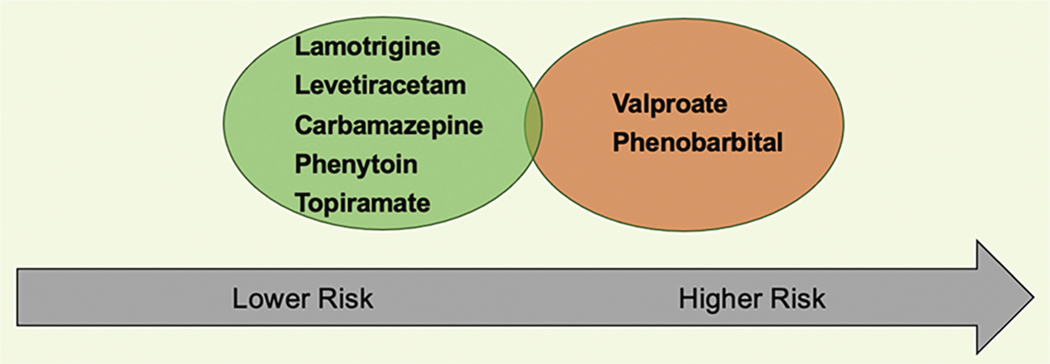
Recent findings: Ongoing multicenter pregnancy registries and studies continue to provide important information on issues related to pregnancy in women with epilepsy. Valproate poses a special risk for malformations and cognitive/behavioral impairments. A few antiseizure medications pose low risks (eg, lamotrigine, levetiracetam), but the risks for many antiseizure medications remain uncertain. Although pregnancy rates differ, a prospective study found no difference in fertility rates between women with epilepsy who were attempting to get pregnant and healthy controls. During pregnancy, folic acid supplementation is important, and a dose greater than 400 mcg/d during early pregnancy (ie, first 12 weeks) is associated with better neurodevelopmental outcome in children of women with epilepsy. Breastfeeding is not harmful and should be encouraged in women with epilepsy even when they are on antiseizure medication treatment.
Summary: Women with epilepsy should be counseled early and regularly about reproductive health. Practitioners should discuss the risks of various obstetric complications; potential anatomic teratogenicity and neurodevelopmental dysfunction related to fetal antiseizure medication exposure; and a plan of care during pregnancy, delivery, and postpartum. Women with epilepsy should also be reassured that the majority of pregnancies are uneventful.
Copyright © 2022 American Academy of Neurology.
Figures
References
-
- Harden CL, Hopp J, Ting TY, et al. Practice parameter update: management issues for women with epilepsy—focus on pregnancy (an evidence-based review): obstetrical complications and change in seizure frequency: report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society. Neurology 2009;73(2):126–132. doi:10.1212/WNL.0b013e3181a6b2f8 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials