

Association of ventilator type with hospital mortality in critically ill patients with SARS-CoV2 infection: a prospective study
- PMID: 35133543
- PMCID: PMC8821831
- DOI: 10.1186/s13613-022-00981-2
Association of ventilator type with hospital mortality in critically ill patients with SARS-CoV2 infection: a prospective study
Abstract
Background: To evaluate the association between ventilator type and hospital mortality in patients with acute respiratory distress syndrome (ARDS) related to COVID-19 (SARS-CoV2 infection), a single-center prospective observational study in France.
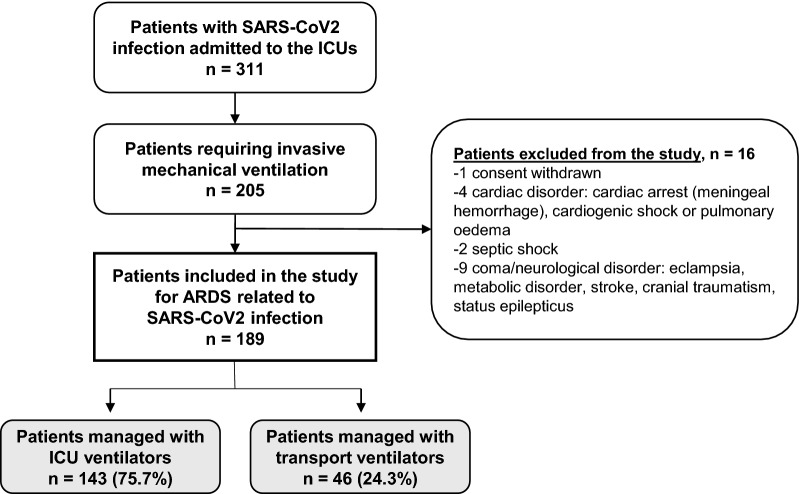
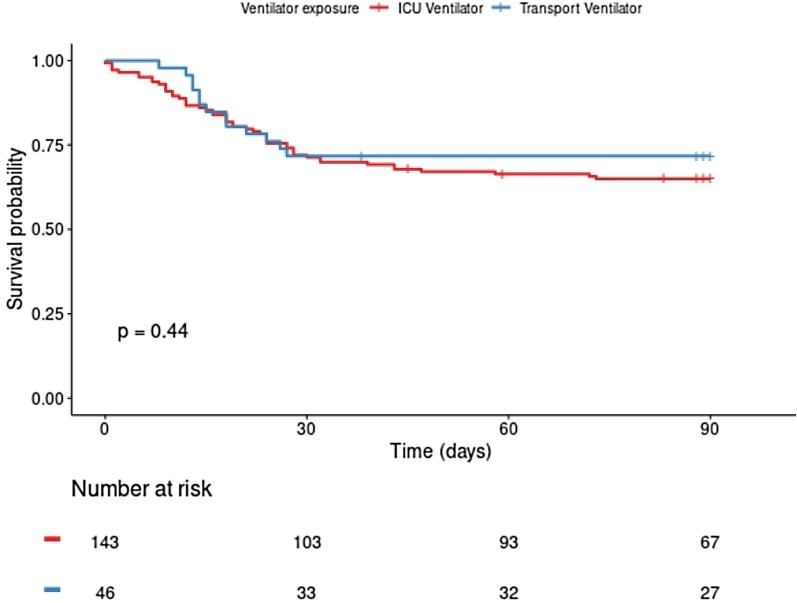
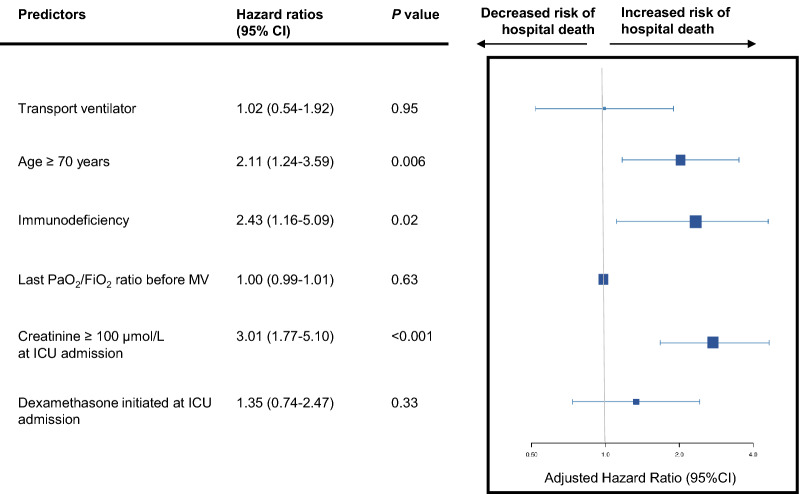
Results: We prospectively included consecutive adults admitted to the intensive care unit (ICU) of a university-affiliated tertiary hospital for ARDS related to proven COVID-19, between March 2020 and July 2021. All patients were intubated. We compared two patient groups defined by whether an ICU ventilator or a less sophisticated ventilator such as a sophisticated turbine-based transport ventilator was used. Kaplan-Meier survival curves were plotted. Cox multivariate regression was performed to identify associations between patient characteristics and hospital mortality. We included 189 patients (140 [74.1%] men) with a median age of 65 years [IQR, 55-73], of whom 61 (32.3%) died before hospital discharge. By multivariate analysis, factors associated with in-hospital mortality were age ≥ 70 years (HR, 2.11; 95% CI, 1.24-3.59; P = 0.006), immunodeficiency (HR, 2.43; 95% CI, 1.16-5.09; P = 0.02) and serum creatinine ≥ 100 µmol/L (HR, 3.01; 95% CI, 1.77-5.10; P < 0.001) but not ventilator type. As compared to conventional ICU (equipped with ICU and anesthesiology ventilators), management in transient ICU (equipped with non-ICU turbine-based ventilators) was associated neither with a longer duration of invasive mechanical ventilation (18 [IQR, 11-32] vs. 21 [13-37] days, respectively; P = 0.39) nor with a longer ICU stay (24 [IQR, 14-40] vs. 27 [15-44] days, respectively; P = 0.44).
Conclusions: In ventilated patients with ARDS due to COVID-19, management in transient ICU equipped with non-ICU sophisticated turbine-based ventilators was not associated with worse outcomes compared to standard ICU, equipped with ICU ventilators. Although our study design is not powered to demonstrate any difference in outcome, our results after adjustment do not suggest any signal of harm when using these transport type ventilators as an alternative to ICU ventilators during COVID-19 surge.
Keywords: COVID-19; ICU; Mortality; Outcomes; Ventilator.
© 2022. The Author(s).
Conflict of interest statement
None of the authors has any competing interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
