

Phase II Study of Copanlisib in Patients With Tumors With PIK3CA Mutations: Results From the NCI-MATCH ECOG-ACRIN Trial (EAY131) Subprotocol Z1F
- PMID: 35133871
- PMCID: PMC9084438
- DOI: 10.1200/JCO.21.01648
Phase II Study of Copanlisib in Patients With Tumors With PIK3CA Mutations: Results From the NCI-MATCH ECOG-ACRIN Trial (EAY131) Subprotocol Z1F
Abstract
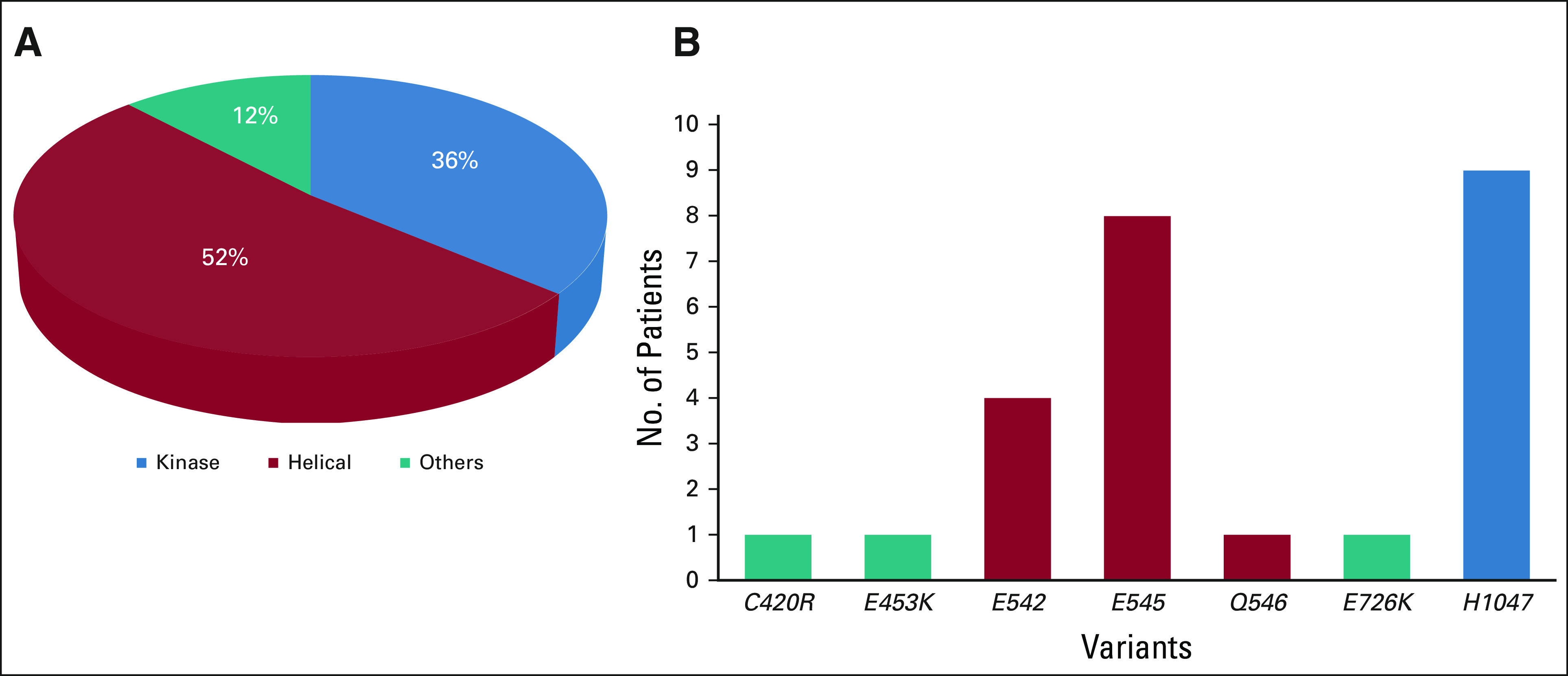
Purpose: Activating mutations in PIK3CA are observed across multiple tumor types. The NCI-MATCH (EAY131) is a tumor-agnostic platform trial that enrolls patients to targeted therapies on the basis of matching genomic alterations. Arm Z1F evaluated copanlisib, an α and δ isoform-specific phosphoinositide 3-kinase (PI3K) inhibitor, in patients with PIK3CA mutations (with or without PTEN loss).
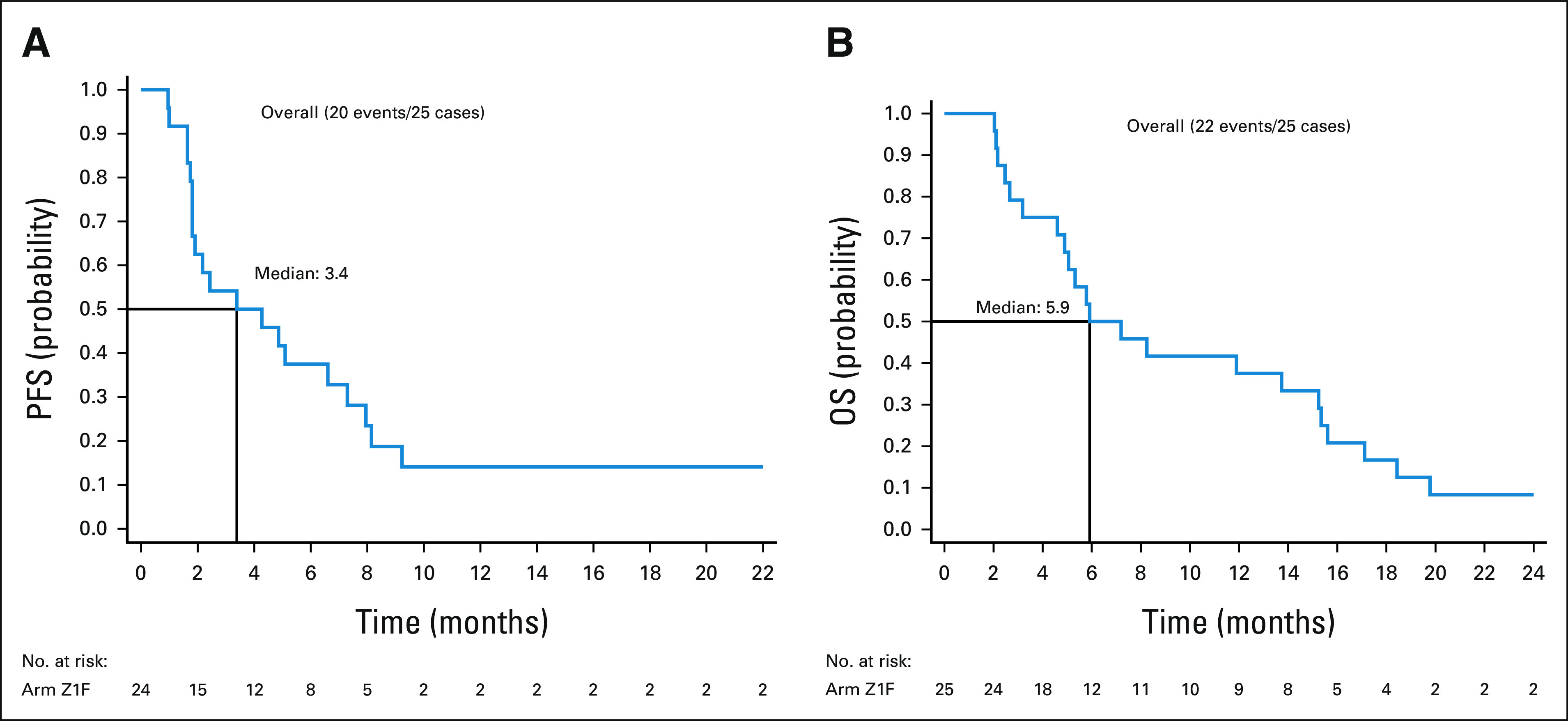
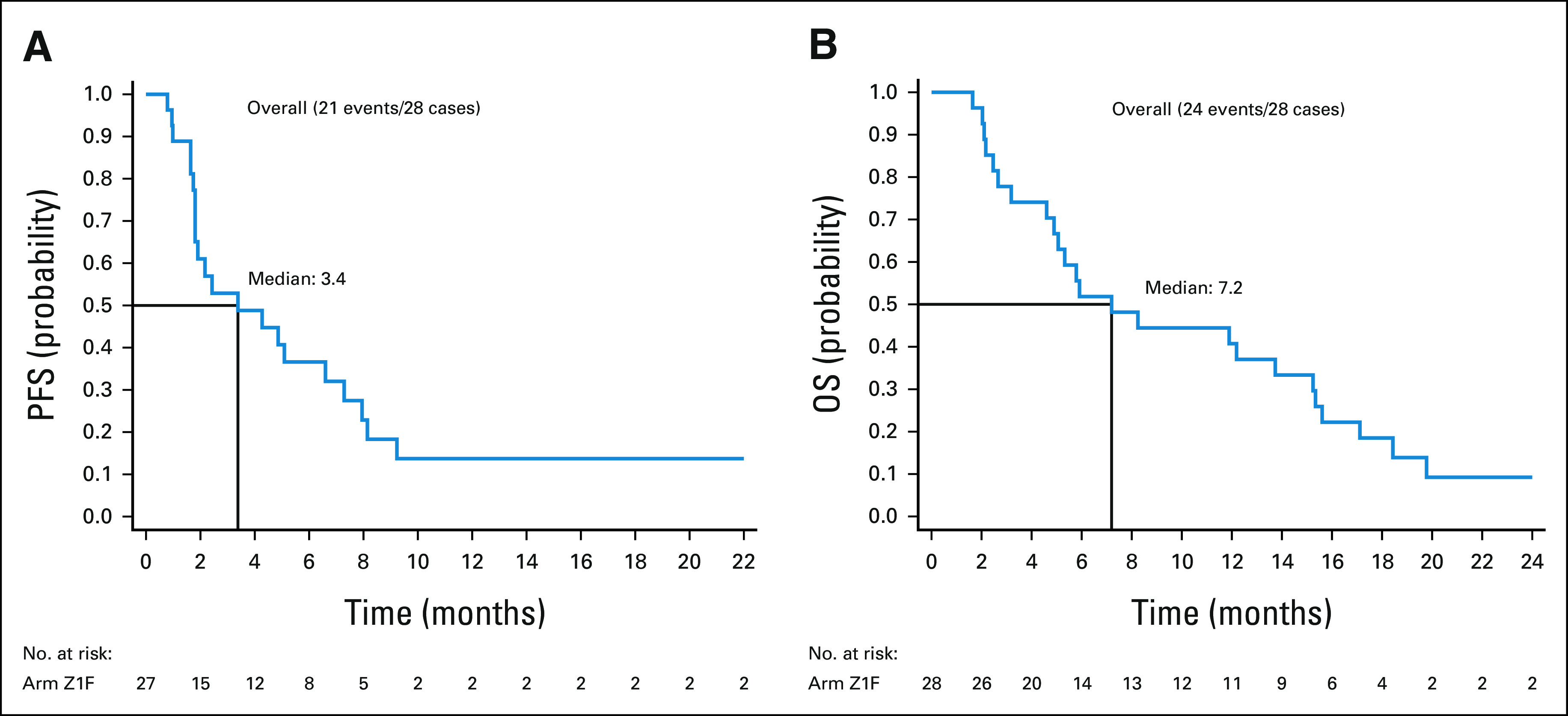
Patients and methods: Patients received copanlisib (60 mg intravenous) once weekly on days 1, 8, and 15 in 28-day cycles until progression or toxicity. Patients with KRAS mutations, human epidermal growth factor receptor 2-positive breast cancers, and lymphomas were excluded. The primary end point was centrally assessed objective response rate (ORR); secondary end points included progression-free survival, 6-month progression-free survival, and overall survival.
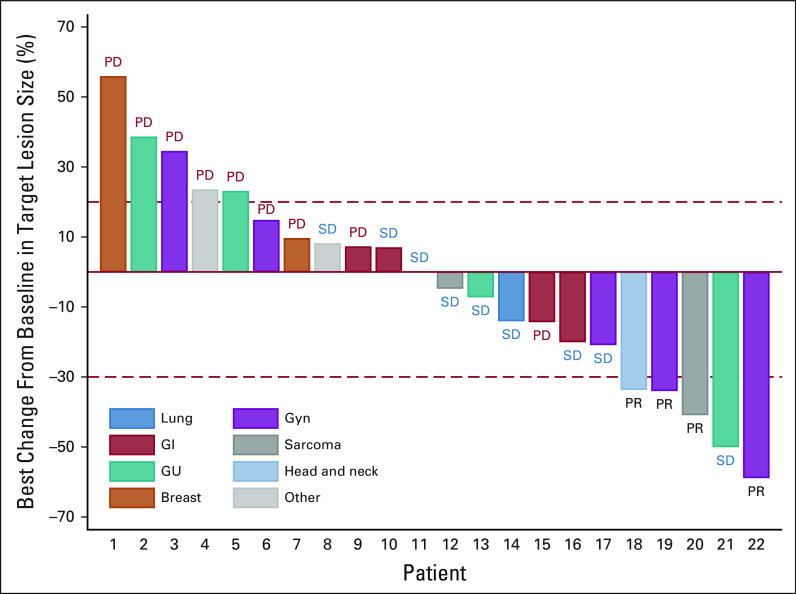
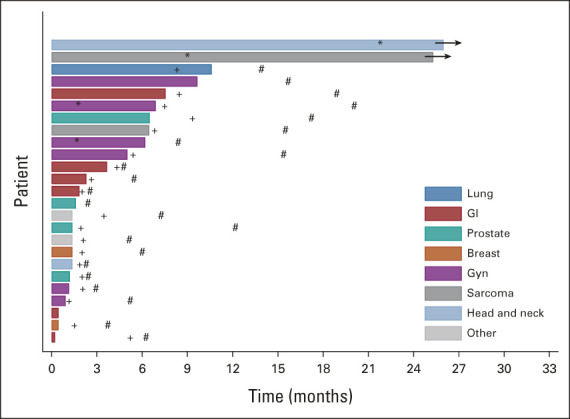
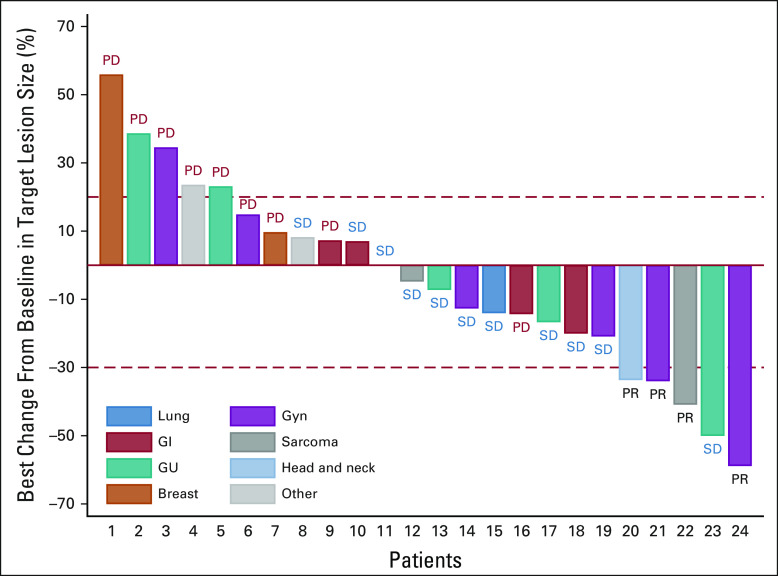
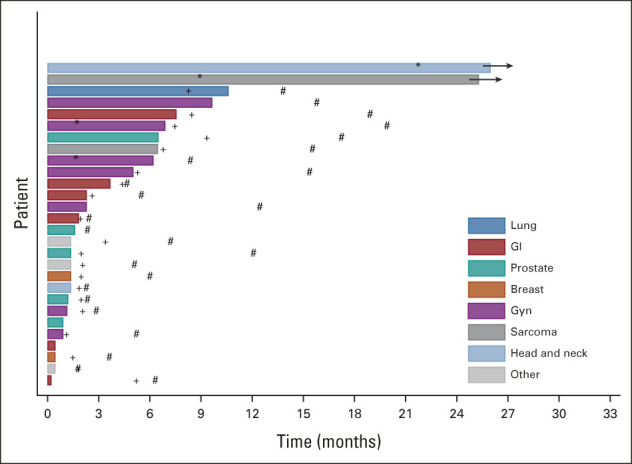
Results: Thirty-five patients were enrolled, and 25 patients were included in the primary efficacy analysis as prespecified in the Protocol. Multiple histologies were enrolled, with gynecologic (n = 6) and gastrointestinal (n = 6) being the most common. Sixty-eight percent of patients had ≥ 3 lines of prior therapy. The ORR was 16% (4 of 25, 90% CI, 6 to 33) with P = .0341 against a null rate of 5%. The most common reason for protocol discontinuation was disease progression (n = 17, 68%). Grade 3/4 toxicities observed were consistent with reported toxicities for PI3K pathway inhibition. Sixteen patients (53%) had grade 3 toxicities, and one patient (3%) had grade 4 toxicity (CTCAE v5.0). Most common toxicities include hyperglycemia (n = 19), fatigue (n = 12), diarrhea (n = 11), hypertension (n = 10), and nausea (n = 10).
Conclusion: The study met its primary end point with an ORR of 16% (P = .0341) with copanlisib showing clinical activity in select tumors with PIK3CA mutation in the refractory setting.
Trial registration: ClinicalTrials.gov NCT02465060.
Conflict of interest statement
Figures


References
-
- Samuels Y, Wang Z, Bardelli A, et al. : High frequency of mutations of the PIK3CA gene in human cancers. Science 304:554, 2004 - PubMed
-
- Andre F, Ciruelos E, Rubovszky G, et al. : Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N Engl J Med 380:1929-1940, 2019 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
