

Exercise-based rehabilitation reduces reinjury following acute lateral ankle sprain: A systematic review update with meta-analysis
- PMID: 35134061
- PMCID: PMC8824326
- DOI: 10.1371/journal.pone.0262023
Exercise-based rehabilitation reduces reinjury following acute lateral ankle sprain: A systematic review update with meta-analysis
Abstract
Research questions: 1) Do exercise-based rehabilitation programs reduce re-injury following acute ankle sprain?; 2) Is rehabilitation effectiveness moderated by the exercise's therapeutic quality, content and volume?
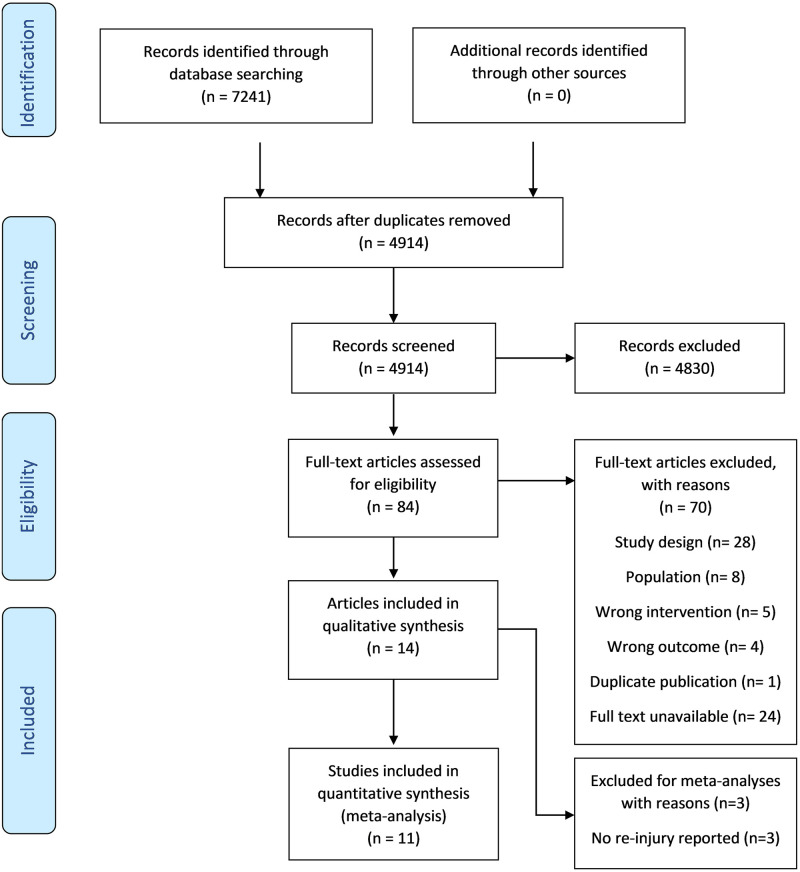
Methods: This systematic review with meta-analysis (PROSPERO: CRD42020210858) included randomized controlled trials in which adults who sustained an acute ankle sprain received exercise-based rehabilitation as an intervention. Databases CINAHL, Web of Science, SPORTDiscus, Cochrane Central Register of Controlled Trials, PEDro and Google Scholar were searched for eligible articles (last search: March 2021). ROB II screening tool by Cochrane was used to assess risk of bias and the i-CONTENT tool was used to assess quality of interventions. Both qualitative analysis and quantitative data synthesis were performed.
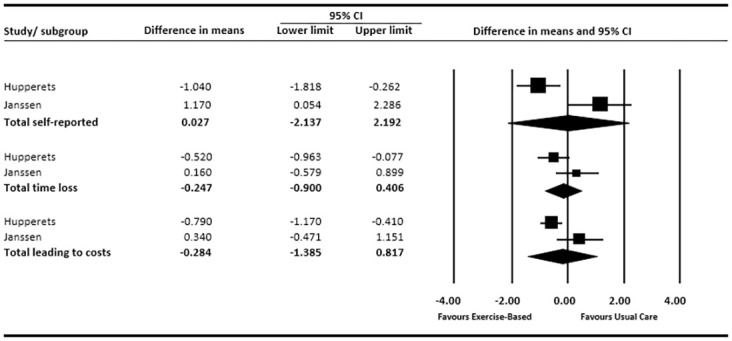
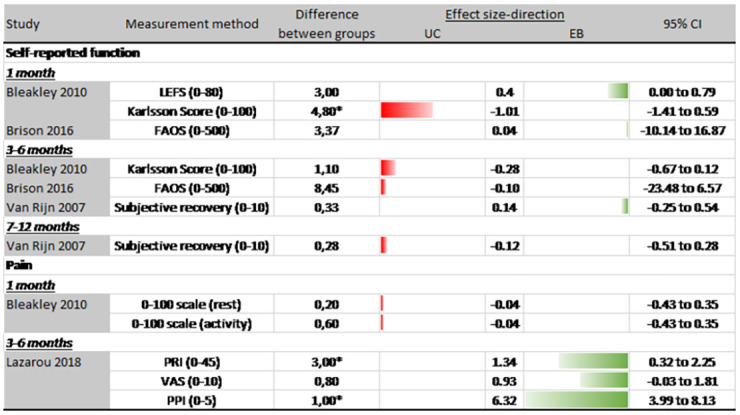
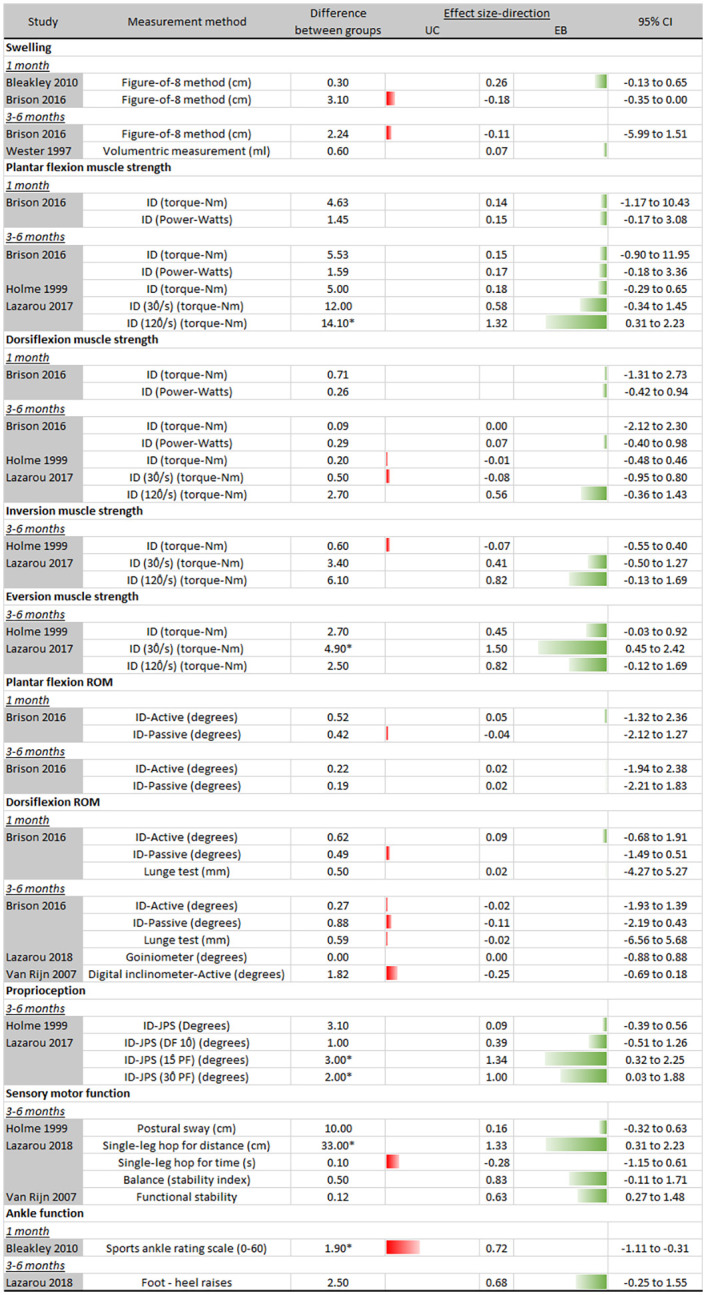
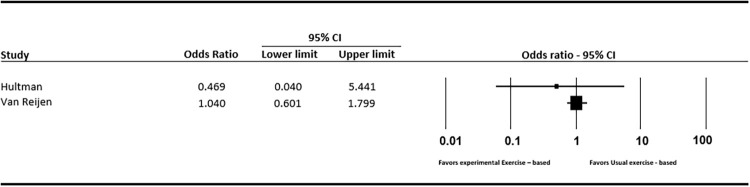
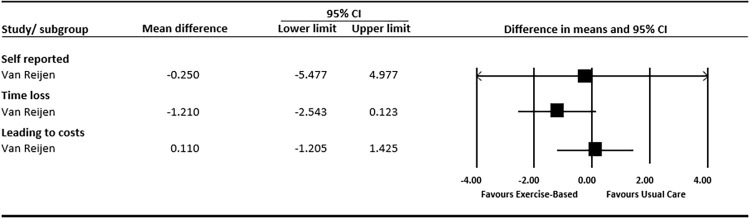
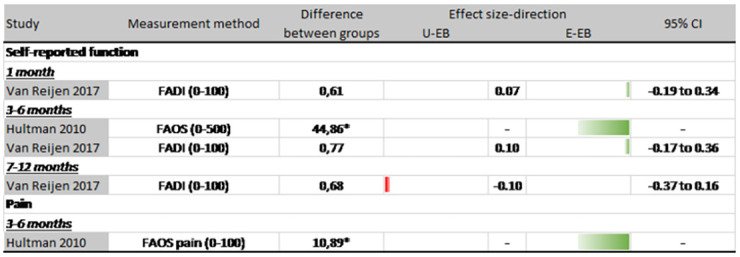
Results: Fourteen randomized controlled trials comprising 2182 participants were included. Five studies were judged overall low risk of bias and i-CONTENT assessment showed poor to moderate therapeutic quality of exercise across all included articles. Pooled data found significant reductions in re-injury prevalence at 12 months, in favour of the exercise-based rehabilitation group vs usual care (OR: 0.60; 95%CI: 0.36 to 0.99). Pooled data for re-injury incidence showed not-significant results (MD: 0.027; 95%CI: -2.14 to 2.19). Meta-regression displayed no statistically significant association between training volume and odds of re-injury (r = -0.00086; SD: 0.00057; 95%CI: -0.00197 to 0.00025). Results from patient-reported outcomes and clinical outcomes were inconclusive at 1 month, 3-6 months and 7-12 months of follow up.
Conclusion: Exercise-based rehabilitation reduces the risk of recurrent ankle sprain compared to usual care, but there is insufficient data to determine the optimal content of exercise-based interventions. Training volume varied considerably across studies but did not affect the odds of sustaining a re-injury. Effects on patient-reported outcomes and clinical outcomes are equivocal. Future research should compare different exercise contents, training volumes and intensities after ankle sprain.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Gribble PA, Bleakley CM, Caulfield BM, Docherty CL, Fourchet F, Fong DT, et al. Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. British journal of sports medicine. 2016;50(24):1496–505. doi: 10.1136/bjsports-2016-096189 - DOI - PubMed
