

Risk of Severe Acute Respiratory Syndrome Coronavirus 2 Acquisition Is Associated With Individual Exposure but Not Community-Level Transmission
- PMID: 35134185
- PMCID: PMC8903329
- DOI: 10.1093/infdis/jiac029
Risk of Severe Acute Respiratory Syndrome Coronavirus 2 Acquisition Is Associated With Individual Exposure but Not Community-Level Transmission
Abstract
Background: Transmission rates after exposure to a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-positive individual within households and healthcare settings varies significantly between studies. Variability in the extent of exposure and community SARS-CoV-2 incidence may contribute to differences in observed rates.
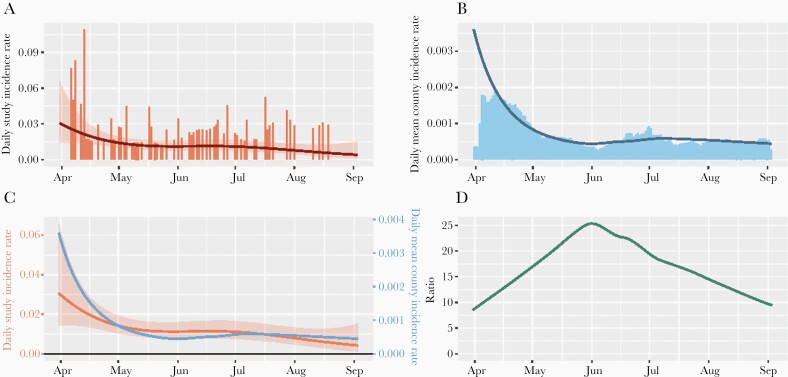
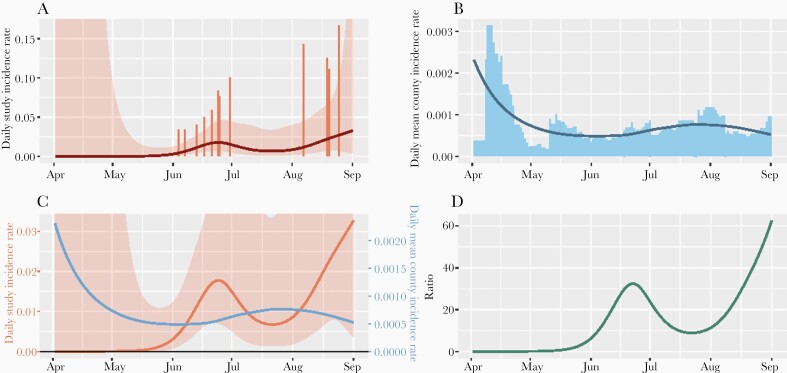
Methods: We examined risk factors for SARS-CoV-2 infection in a randomized controlled trial of hydroxychloroquine as postexposure prophylaxis. Study procedures included standardized questionnaires at enrollment and daily self-collection of midturbinate swabs for SARS-CoV-2 polymerase chain reaction testing. County-level incidence was modeled using federally sourced data. Relative risks and 95% confidence intervals were calculated using modified Poisson regression.
Results: Eighty-six of 567 (15.2%) household/social contacts and 12 of 122 (9.8%) healthcare worker contacts acquired SARS-CoV-2 infection. Exposure to 2 suspected index cases (vs 1) significantly increased risk for both household/social contacts (relative risk [RR], 1.86) and healthcare workers (RR, 8.18). Increased contact time also increased risk for healthcare workers (3-12 hours: RR, 7.82, >12 hours: RR, 11.81, vs ≤2 hours), but not for household/social contacts. County incidence did not impact risk.
Conclusions: In our study, increased exposure to SARS-CoV-2 within household or healthcare settings led to higher risk of infection, but elevated community incidence did not. This reinforces the importance of interventions to decrease transmission in close contact settings.
Keywords: COVID-19; SARS-CoV-2; healthcare worker transmission; household transmission.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Wolfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020; 581:465–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
