

Effects of personalized diets by prediction of glycemic responses on glycemic control and metabolic health in newly diagnosed T2DM: a randomized dietary intervention pilot trial
- PMID: 35135549
- PMCID: PMC8826661
- DOI: 10.1186/s12916-022-02254-y
Effects of personalized diets by prediction of glycemic responses on glycemic control and metabolic health in newly diagnosed T2DM: a randomized dietary intervention pilot trial
Abstract
Background: Dietary modifications are crucial for managing newly diagnosed type 2 diabetes mellitus (T2DM) and preventing its health complications, but many patients fail to achieve clinical goals with diet alone. We sought to evaluate the clinical effects of a personalized postprandial-targeting (PPT) diet on glycemic control and metabolic health in individuals with newly diagnosed T2DM as compared to the commonly recommended Mediterranean-style (MED) diet.
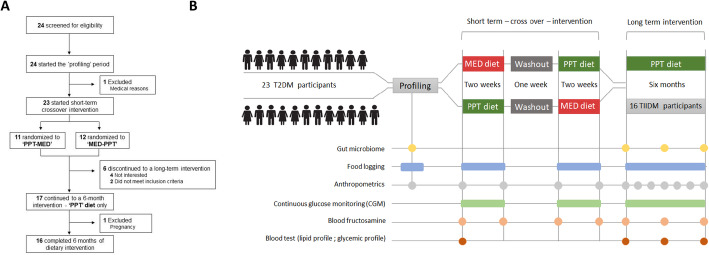
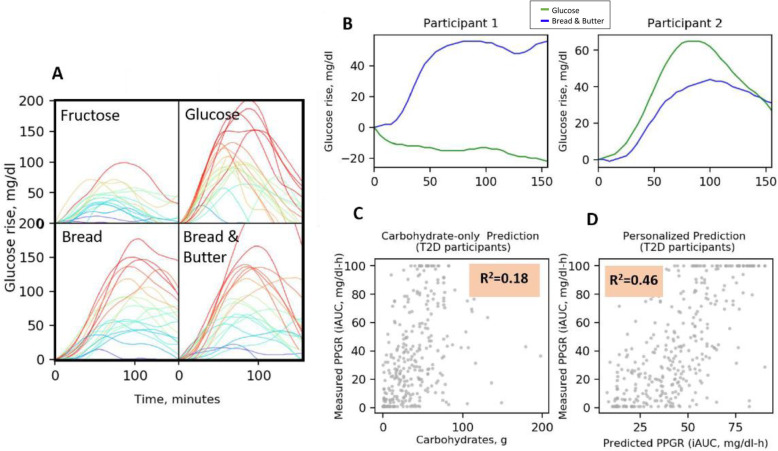
Methods: We enrolled 23 adults with newly diagnosed T2DM (aged 53.5 ± 8.9 years, 48% males) for a randomized crossover trial of two 2-week-long dietary interventions. Participants were blinded to their assignment to one of the two sequence groups: either PPT-MED or MED-PPT diets. The PPT diet relies on a machine learning algorithm that integrates clinical and microbiome features to predict personal postprandial glucose responses (PPGR). We further evaluated the long-term effects of PPT diet on glycemic control and metabolic health by an additional 6-month PPT intervention (n = 16). Participants were connected to continuous glucose monitoring (CGM) throughout the study and self-recorded dietary intake using a smartphone application.
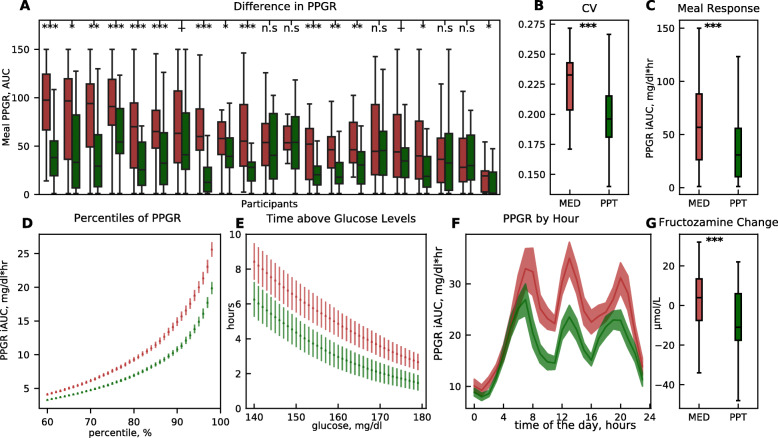
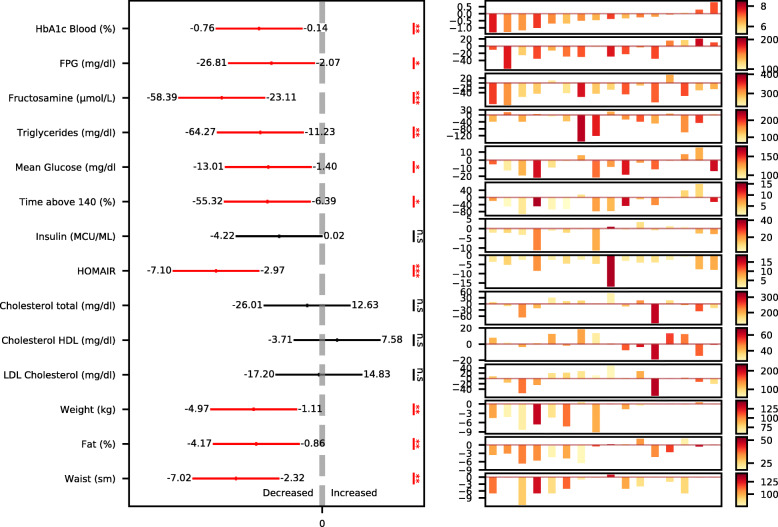
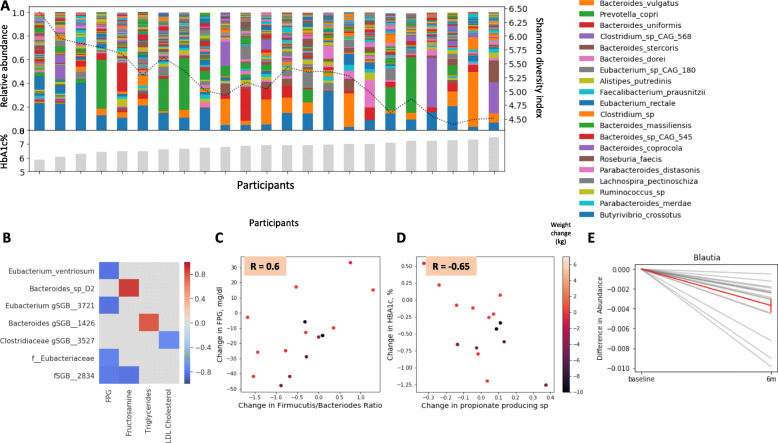
Results: In the crossover intervention, the PPT diet lead to significant lower levels of CGM-based measures as compared to the MED diet, including average PPGR (mean difference between diets, - 19.8 ± 16.3 mg/dl × h, p < 0.001), mean glucose (mean difference between diets, - 7.8 ± 5.5 mg/dl, p < 0.001), and daily time of glucose levels > 140 mg/dl (mean difference between diets, - 2.42 ± 1.7 h/day, p < 0.001). Blood fructosamine also decreased significantly more during PPT compared to MED intervention (mean change difference between diets, - 16.4 ± 37 μmol/dl, p < 0.0001). At the end of 6 months, the PPT intervention leads to significant improvements in multiple metabolic health parameters, among them HbA1c (mean ± SD, - 0.39 ± 0.48%, p < 0.001), fasting glucose (- 16.4 ± 24.2 mg/dl, p = 0.02) and triglycerides (- 49 ± 46 mg/dl, p < 0.001). Importantly, 61% of the participants exhibited diabetes remission, as measured by HbA1c < 6.5%. Finally, some clinical improvements were significantly associated with gut microbiome changes per person.
Conclusion: In this crossover trial in subjects with newly diagnosed T2DM, a PPT diet improved CGM-based glycemic measures significantly more than a Mediterranean-style MED diet. Additional 6-month PPT intervention further improved glycemic control and metabolic health parameters, supporting the clinical efficacy of this approach.
Trial registration: ClinicalTrials.gov number, NCT01892956.
Keywords: Dietary intervention; Gut microbiome; Personalized nutrition; Postprandial glucose responses; Type 2 diabetes mellitus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Neeland IJ, Patel KV. Diabetes. In: Biomarkers in cardiovascular disease. Elsevier; 2019. p. 41–51.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
