

Development of a convolutional neural network for the identification and the measurement of the median nerve on ultrasound images acquired at carpal tunnel level
- PMID: 35135598
- PMCID: PMC8822696
- DOI: 10.1186/s13075-022-02729-6
Development of a convolutional neural network for the identification and the measurement of the median nerve on ultrasound images acquired at carpal tunnel level
Abstract
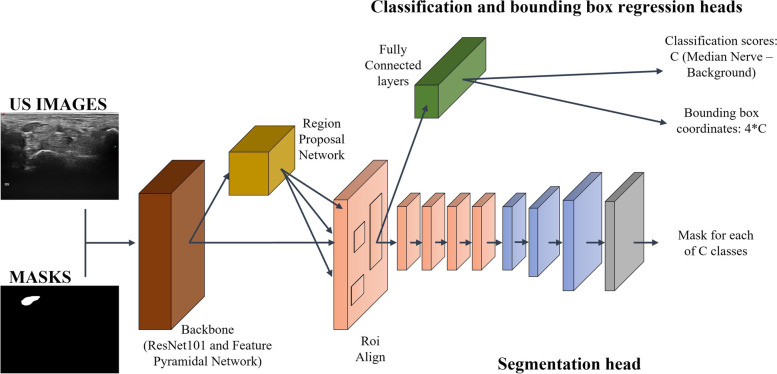
Background: Deep learning applied to ultrasound (US) can provide a feedback to the sonographer about the correct identification of scanned tissues and allows for faster and standardized measurements. The most frequently adopted parameter for US diagnosis of carpal tunnel syndrome is the increasing of the cross-sectional area (CSA) of the median nerve. Our aim was to develop a deep learning algorithm, relying on convolutional neural networks (CNNs), for the localization and segmentation of the median nerve and the automatic measurement of its CSA on US images acquired at the proximal inlet of the carpal tunnel.
Methods: Consecutive patients with rheumatic and musculoskeletal disorders were recruited. Transverse US images were acquired at the carpal tunnel inlet, and the CSA was manually measured. Anatomical variants were registered. The dataset consisted of 246 images (157 for training, 40 for validation, and 49 for testing) from 103 patients each associated with manual annotations of the nerve boundary. A Mask R-CNN, state-of-the-art CNN for image semantic segmentation, was trained on this dataset to accurately localize and segment the median nerve section. To evaluate the performances on the testing set, precision (Prec), recall (Rec), mean average precision (mAP), and Dice similarity coefficient (DSC) were computed. A sub-analysis excluding anatomical variants was performed. The CSA was automatically measured by the algorithm.
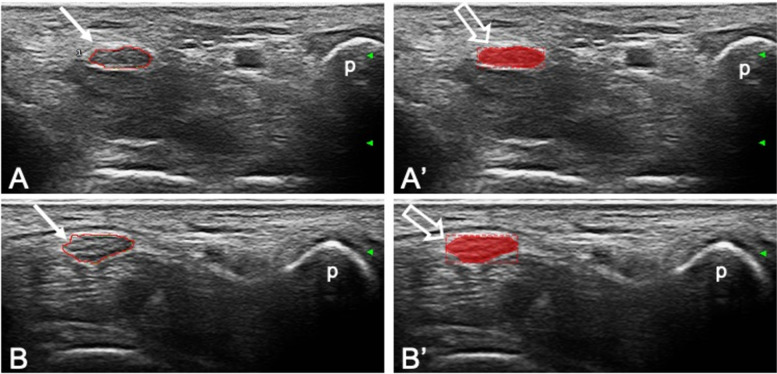
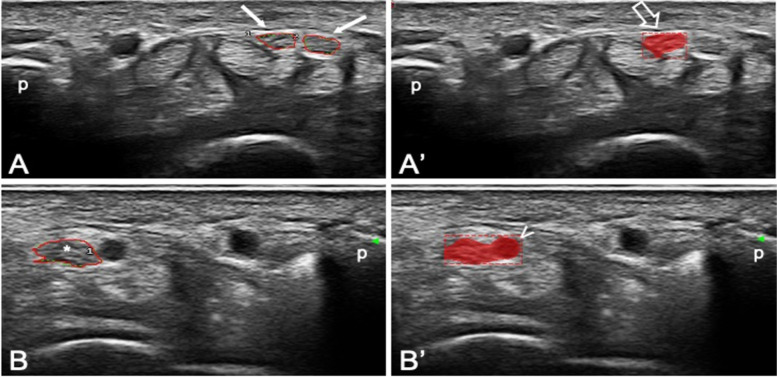
Results: The algorithm correctly identified the median nerve in 41/49 images (83.7%) and in 41/43 images (95.3%) excluding anatomical variants. The following metrics were obtained (with and without anatomical variants, respectively): Prec 0.86 ± 0.33 and 0.96 ± 0.18, Rec 0.88 ± 0.33 and 0.98 ± 0.15, mAP 0.88 ± 0.33 and 0.98 ± 0.15, and DSC 0.86 ± 0.19 and 0.88 ± 0.19. The agreement between the algorithm and the sonographer CSA measurements was excellent [ICC 0.97 (0.94-0.98)].
Conclusions: The developed algorithm has shown excellent performances, especially if excluding anatomical variants. Future research should aim at expanding the US image dataset including a wider spectrum of normal anatomy and pathology. This deep learning approach has shown very high potentiality for a fully automatic support for US assessment of carpal tunnel syndrome.
© 2022. The Author(s).
Conflict of interest statement
E.F. has received speaking fees from Abbvie, BMS, Janssen, Lilly, MSD, Novartis, Roche, Pfizer, and UCB Pharma. W.G. has received speaking fees from AbbVie, Celgene, Grünenthal, Pfizer, and UCB Pharma. All other authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
