

doi: 10.2215/CJN.14201021.
Epub 2022 Feb 8.
Syndromes of Pseudo-Hyperaldosteronism
Affiliations
- PMID: 35135780
- PMCID: PMC8993470
- DOI: 10.2215/CJN.14201021
Item in Clipboard
Syndromes of Pseudo-Hyperaldosteronism
Clin J Am Soc Nephrol.
2022 Apr.
No abstract available
Keywords: aldosterone; hypertension; hypokalemia.
Figures
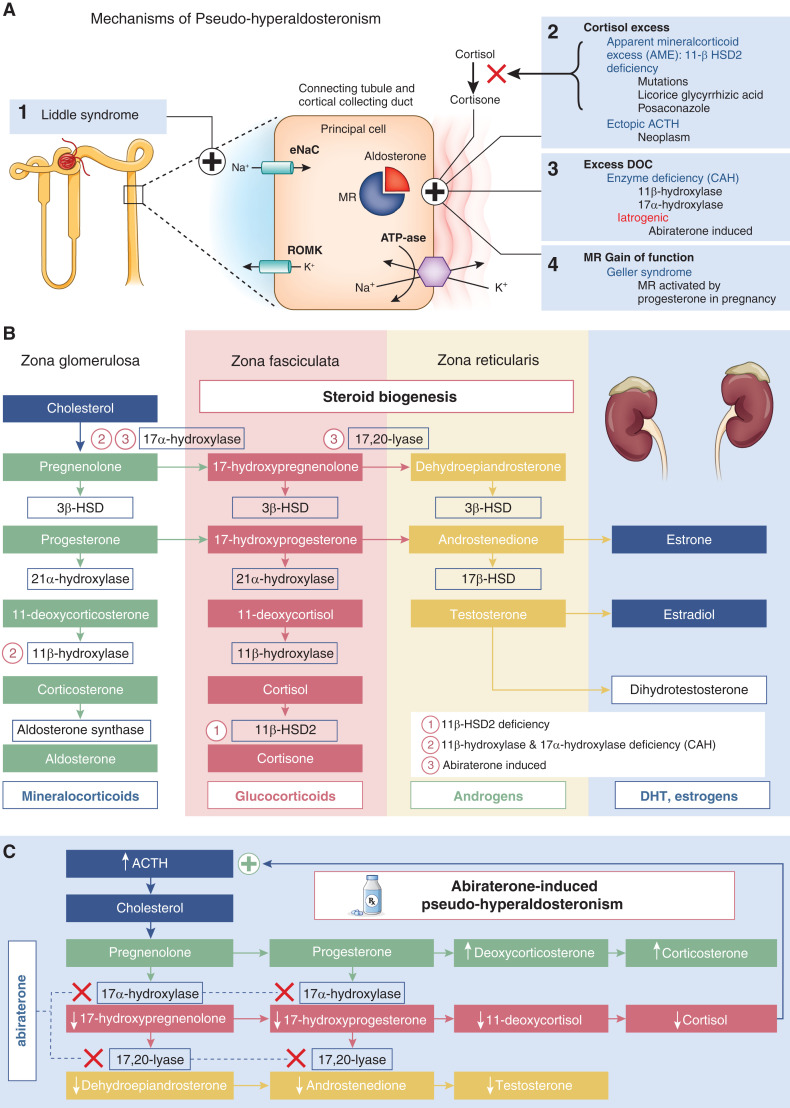
Mechanisms of pseudo-hyperaldosteronism and steroid biogenesis pathways. (A) Mechanisms of pseudo-hyperaldosteronism. (1) Primary channelopathy. Liddle syndrome, an autosomal dominant mutation of the gene encoding for the epithelial sodium channel (ENaC) causing constitutive ENaC activation, leads to excessive sodium (Na+) reabsorption in the distal tubule. (2) Excess cortisol activation of the mineralocorticoid receptor (MR) is from (a) apparent mineralocorticoid excess due to 11β-hydroxysteroid dehydrogenase type 2 (11-βHSD2) deficiency from an autosomal recessive mutation or ingestions, like black licorice (glicyrrhizic acid), posaconazole, or itraconazole, which prevent conversion of cortisol to the inert form cortisone, or (b) ectopic adrenocorticotrophic hormone (ACTH) that stimulates excess cortisol secretion exceeding 11-βHSD2 deactivation capacity. (3) Excess deoxycorticosterone (DOC) activating the MR is from (a) congenital adrenal hyperplasia (CAH), an autosomal recessive mutation causing 11β-hydroxylase and 17α-hydroxylase deficiencies during steroid biogenesis, or (b) abiraterone-induced inhibition of 17α-hydroxylase and C17,20-lyase resulting in low testosterone and cortisol levels, loss of ACTH inhibition, and subsequent DOC excess. (4) MR gain of function. Geller syndrome, an autosomal dominant mutation causing constitutive activation of MR by progesterone, was unmasked during pregnancy. (B) Steroid biogenesis pathways. (C) Mechanism of abiraterone-induced pseudo-hyperaldosteronism. DHT, dihydrotestosterone; 3β-HSD, 3β-hydroxysteroid dehydrogenase; 17β-HSD, 17β-hydroxysteroid dehydrogenase; ROMK, renal outer medullary potassium channel.
References
-
- Palmer BF: A physiologic-based approach to the evaluation of a patient with hypokalemia. Am J Kidney Dis 56: 1184–1190, 2010 - PubMed
-
- Weinberger MH, Fineberg NS: The diagnosis of primary aldosteronism and separation of two major subtypes. Arch Intern Med 153: 2125–2129, 1993 - PubMed
-
- Nussberger J: Investigating mineralocorticoid hypertension. J Hypertens Suppl 21: S25–S30, 2003 - PubMed
-
- Beck KR, Telisman L, van Koppen CJ, Thompson GR 3rd, Odermatt A: Molecular mechanisms of posaconazole- and itraconazole-induced pseudohyperaldosteronism and assessment of other systemically used azole antifungals. J Steroid Biochem Mol Biol 199: 105605, 2020 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
