

The CCEDRRN COVID-19 Mortality Score to predict death among nonpalliative patients with COVID-19 presenting to emergency departments: a derivation and validation study
- PMID: 35135824
- PMCID: PMC9259439
- DOI: 10.9778/cmajo.20210243
The CCEDRRN COVID-19 Mortality Score to predict death among nonpalliative patients with COVID-19 presenting to emergency departments: a derivation and validation study
Abstract
Background: Predicting mortality from COVID-19 using information available when patients present to the emergency department can inform goals-of-care decisions and assist with ethical allocation of critical care resources. The study objective was to develop and validate a clinical score to predict emergency department and in-hospital mortality among consecutive nonpalliative patients with COVID-19; in this study, we define palliative patients as those who do not want resuscitative measures, such as intubation, intensive care unit care or cardiopulmonary resuscitation.
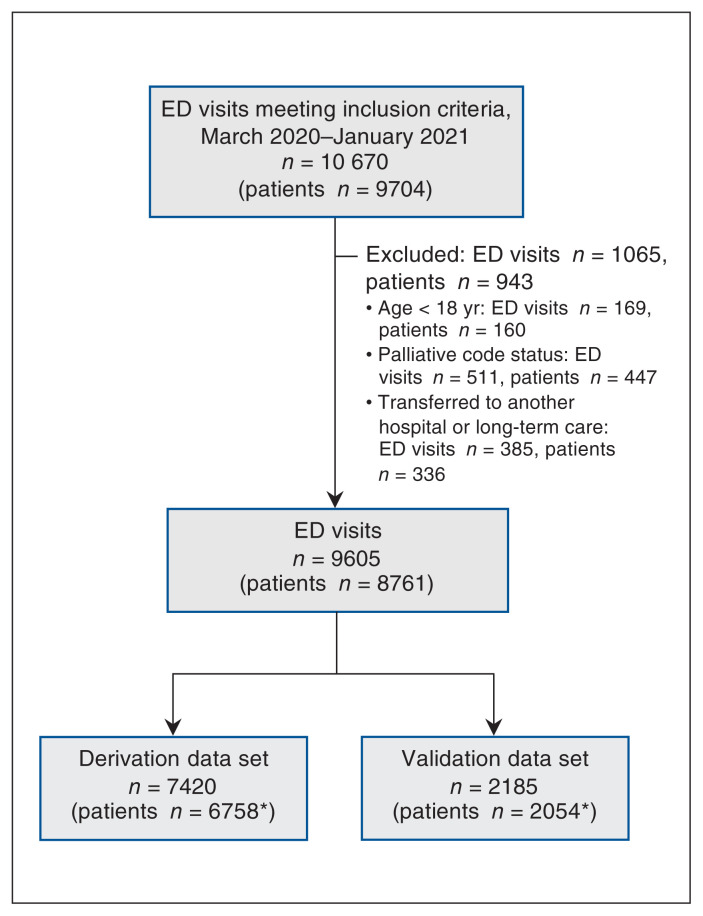
Methods: This derivation and validation study used observational cohort data recruited from 46 hospitals in 8 Canadian provinces participating in the Canadian COVID-19 Emergency Department Rapid Response Network (CCEDRRN). We included adult (age ≥ 18 yr) nonpalliative patients with confirmed COVID-19 who presented to the emergency department of a participating site between Mar. 1, 2020, and Jan. 31, 2021. We randomly assigned hospitals to derivation or validation, and prespecified clinical variables as candidate predictors. We used logistic regression to develop the score in a derivation cohort and examined its performance in predicting emergency department and in-hospital mortality in a validation cohort.
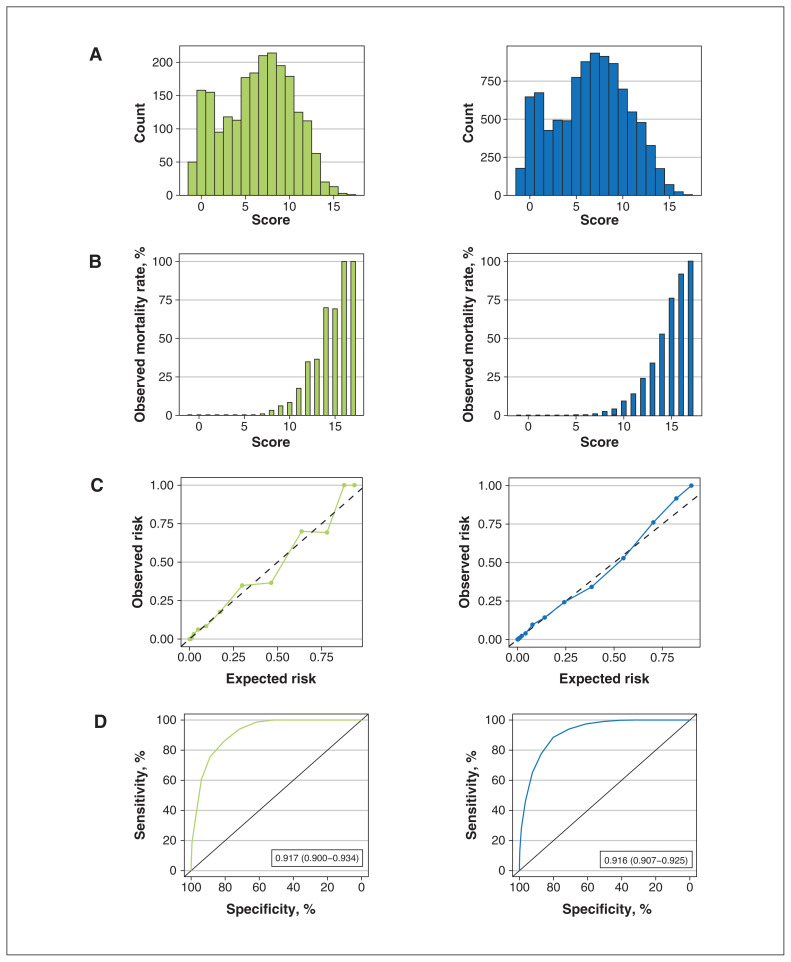
Results: Of 8761 eligible patients, 618 (7.0%) died. The CCEDRRN COVID-19 Mortality Score included age, sex, type of residence, arrival mode, chest pain, severe liver disease, respiratory rate and level of respiratory support. The area under the curve was 0.92 (95% confidence interval [CI] 0.90-0.93) in derivation and 0.92 (95% CI 0.90-0.93) in validation. The score had excellent calibration. These results suggest that scores of 6 or less would categorize patients as being at low risk for in-hospital death, with a negative predictive value of 99.9%. Patients in the low-risk group had an in-hospital mortality rate of 0.1%. Patients with a score of 15 or higher had an observed mortality rate of 81.0%.
Interpretation: The CCEDRRN COVID-19 Mortality Score is a simple score that can be used for level-of-care discussions with patients and in situations of critical care resource constraints to accurately predict death using variables available on emergency department arrival. The score was derived and validated mostly in unvaccinated patients, and before variants of concern were circulating widely and newer treatment regimens implemented in Canada.
Study registration: ClinicalTrials.gov, no. NCT04702945.
© 2022 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Rosenbaum L. Facing COVID-19 in Italy: ethics, logistics, and therapeutics on the epidemic’s front line. N Engl J Med. 2020;382:1873–5. - PubMed
-
- Maves RC, Downar J, Dichter JR, et al. ACCP Task Force for Mass Critical Care. Triage of scarce critical care resources in COVID-19 an implementation guide for regional allocation: an expert panel report of the Task Force for Mass Critical Care and the American College of Chest Physicians. Chest. 2020;158:212–25. - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical