A joint convolutional-recurrent neural network with an attention mechanism for detecting intracranial hemorrhage on noncontrast head CT
- PMID: 35136123
- PMCID: PMC8826390
- DOI: 10.1038/s41598-022-05872-x
A joint convolutional-recurrent neural network with an attention mechanism for detecting intracranial hemorrhage on noncontrast head CT
Abstract
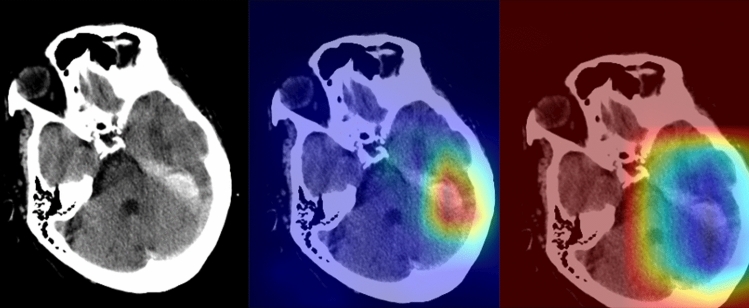
To investigate the performance of a joint convolutional neural networks-recurrent neural networks (CNN-RNN) using an attention mechanism in identifying and classifying intracranial hemorrhage (ICH) on a large multi-center dataset; to test its performance in a prospective independent sample consisting of consecutive real-world patients. All consecutive patients who underwent emergency non-contrast-enhanced head CT in five different centers were retrospectively gathered. Five neuroradiologists created the ground-truth labels. The development dataset was divided into the training and validation set. After the development phase, we integrated the deep learning model into an independent center's PACS environment for over six months for assessing the performance in a real clinical setting. Three radiologists created the ground-truth labels of the testing set with a majority voting. A total of 55,179 head CT scans of 48,070 patients, 28,253 men (58.77%), with a mean age of 53.84 ± 17.64 years (range 18-89) were enrolled in the study. The validation sample comprised 5211 head CT scans, with 991 being annotated as ICH-positive. The model's binary accuracy, sensitivity, and specificity on the validation set were 99.41%, 99.70%, and 98.91, respectively. During the prospective implementation, the model yielded an accuracy of 96.02% on 452 head CT scans with an average prediction time of 45 ± 8 s. The joint CNN-RNN model with an attention mechanism yielded excellent diagnostic accuracy in assessing ICH and its subtypes on a large-scale sample. The model was seamlessly integrated into the radiology workflow. Though slightly decreased performance, it provided decisions on the sample of consecutive real-world patients within a minute.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures