

Uterine bleeding: how understanding endometrial physiology underpins menstrual health
- PMID: 35136207
- PMCID: PMC9098793
- DOI: 10.1038/s41574-021-00629-4
Uterine bleeding: how understanding endometrial physiology underpins menstrual health
Abstract
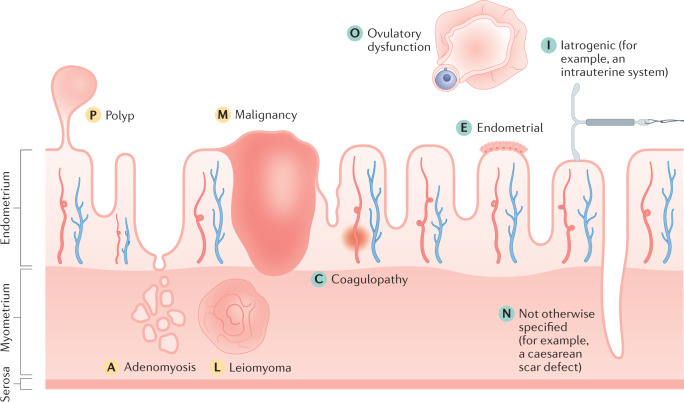
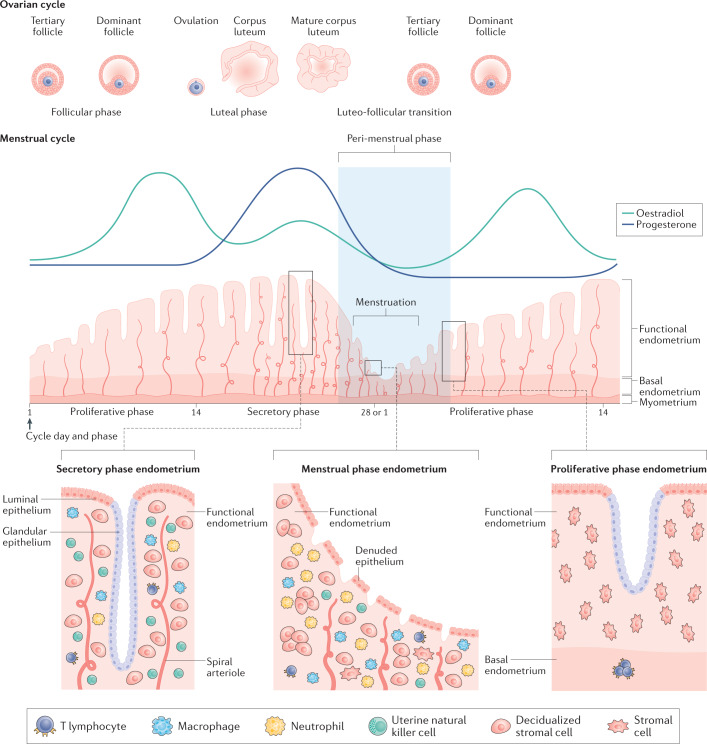
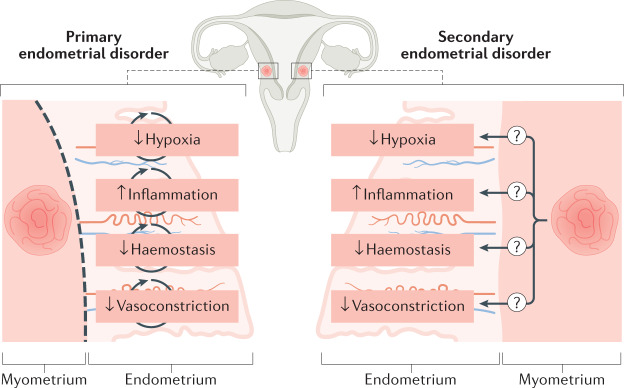
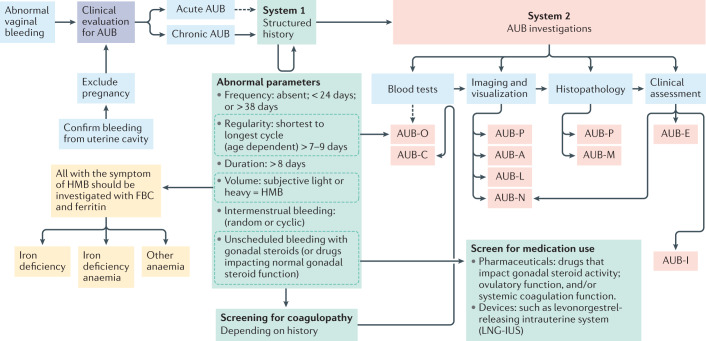
Menstruation is a physiological process that is typically uncomplicated. However, up to one third of women globally will be affected by abnormal uterine bleeding (AUB) at some point in their reproductive years. Menstruation (that is, endometrial shedding) is a fine balance between proliferation, decidualization, inflammation, hypoxia, apoptosis, haemostasis, vasoconstriction and, finally, repair and regeneration. An imbalance in any one of these processes can lead to the abnormal endometrial phenotype of AUB. Poor menstrual health has a negative impact on a person's physical, mental, social, emotional and financial well-being. On a global scale, iron deficiency and iron deficiency anaemia are closely linked with AUB, and are often under-reported and under-recognized. The International Federation of Gynecology and Obstetrics have produced standardized terminology and a classification system for the causes of AUB. This standardization will facilitate future research endeavours, diagnosis and clinical management. In a field where no new medications have been developed for over 20 years, emerging technologies are paving the way for a deeper understanding of the biology of the endometrium in health and disease, as well as opening up novel diagnostic and management avenues.
© 2022. Springer Nature Limited.
Conflict of interest statement
H.O.D.C. has received clinical research support for laboratory consumables and staff from Bayer AG, and provides consultancy advice (but with no personal remuneration) to Bayer AG, PregLem SA, Gedeon Richter, Vifor Pharma UK Ltd, AbbVie Inc. and Myovant Sciences GmbH. H.O.D.C. receives royalties from UpToDate for an article on abnormal uterine bleeding. V.J. receives salary and research consumables support from Wellbeing of Women (WoW). R.R.C. has been supported as a clinical research fellow by Bayer AG. J.A.M. receives salary and research consumables support from The Wellcome Trust.
Figures
References
-
- National Collaborating Centre for Women’s and Children’s Health. Heavy menstrual bleeding (Ch. 3). https://www.nice.org.uk/guidance/ng88/evidence/full-guideline-pdf-478229... (2007).
-
- Royal College of Obstetricians and Gynaecologists. National heavy menstrual bleeding audit final Report (Ch. 1). https://www.rcog.org.uk/globalassets/documents/guidelines/research--audi... (2014).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
