

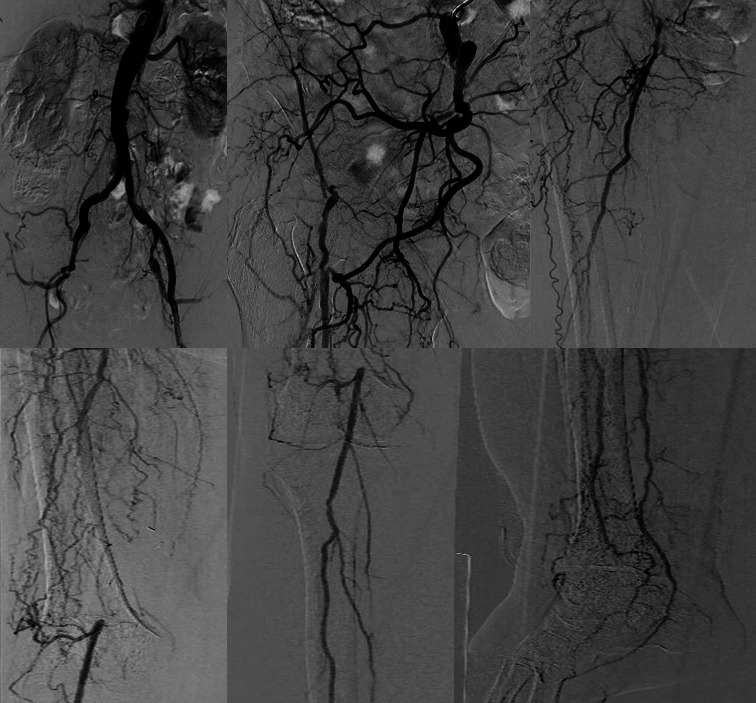
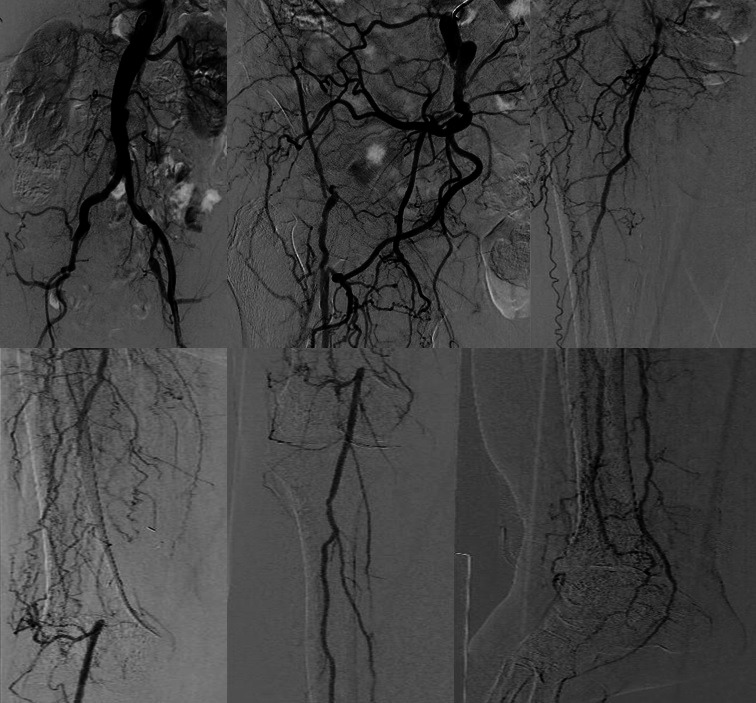
Complex multilevel and multivessel endovascular revascularization through an occluded femoral-popliteal bypass in a patient with chronic limb threatening ischemia
- PMID: 35136404
- PMCID: PMC8786082
- DOI: 10.1590/1677-5449.210057
Complex multilevel and multivessel endovascular revascularization through an occluded femoral-popliteal bypass in a patient with chronic limb threatening ischemia
Abstract
Chronic limb-threatening ischemia (CLTI) represents the end stage of peripheral artery disease, a problem of growing prevalence and increased health care costs around the globe. CLTI is a highly morbid disease, incurring significant mortality, limb loss, pain, and diminished health-related quality of life. The major cause of non-traumatic lower extremity amputation are related to diabetes and CLTI. Between 2% to 3% of patients with peripheral artery disease present with a severe case of CLTI, a condition that is correlated with multilevel and multivessel arterial disease, calcification, and chronic total occlusions. Multiple technical strategies to successfully cross long occlusions in arterial segments have been described. Recanalization can be performed using endoluminal, subintimal, and retrograde techniques. We report a case of complex multilevel and multivessel endovascular revascularization through an occluded femoro-popliteal bypass in a patient with CLTI.
Resumen: La isquemia crónica con amenaza para las extremidades inferiores (ICAEI) representa el estadio final de la enfermedad arterial periférica, un problema de prevalencia creciente que conlleva el aumento de los costos de salud en todo el mundo. La ICAEI es una enfermedad con elevada morbilidad, generando mortalidad significativa, pérdida de miembros, dolor y disminución de la calidad de vida. La principal causa de amputaciones no-traumáticas de miembros inferiores está relacionada a la diabetes y a la ICAEI. Entre un 2% y 3% de los pacientes con enfermedad arterial periférica se presentan con un caso grave de ICAEI, condición que se correlaciona con enfermedad arterial multinivel y multiarterial, calcificación y oclusiones totales crónicas. Se describieron varias estrategias técnicas para cruzar con éxito largas oclusiones en segmentos arteriales. Se puede realizar la recanalización utilizando técnicas endoluminales, subintimales y retrógradas. Relatamos un caso de revascularización endovascular compleja multinivel y multiarterial a través de un bypass fémoro-poplíteo en una paciente con ICAEI.
Keywords: chronic limb-threatening ischemia; endovascular; retrograde approach; subintimal angioplasty.
Copyright© 2021 The authors.
Conflict of interest statement
Conflicts of interest: No conflicts of interest declared concerning the publication of this article.
Figures



Similar articles
-
Effectiveness of combined superficial femoral artery endovascular therapy with popliteal-to-distal bypass: A paradigm shift in surgical open bypass for chronic limb-threatening ischemia.Vascular. 2021 Dec;29(6):905-912. doi: 10.1177/1708538120981224. Epub 2020 Dec 21. Vascular. 2021. PMID: 33349196
-
Trans-popliteal hybrid retrograde technique for revascularization of chronic total occlusions of the superficial femoral artery.Vascular. 2021 Aug;29(4):582-588. doi: 10.1177/1708538120966130. Epub 2020 Oct 22. Vascular. 2021. PMID: 33086943
-
Stenting for peripheral artery disease of the lower extremities: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(18):1-88. Epub 2010 Sep 1. Ont Health Technol Assess Ser. 2010. PMID: 23074395 Free PMC article.
-
A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia.Eur J Vasc Endovasc Surg. 2019 Jul;58(1S):S110-S119. doi: 10.1016/j.ejvs.2019.04.013. Epub 2019 Jun 17. Eur J Vasc Endovasc Surg. 2019. PMID: 31221539
-
A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia.J Vasc Surg. 2019 Jun;69(6S):126S-136S. doi: 10.1016/j.jvs.2018.01.071. Epub 2019 May 28. J Vasc Surg. 2019. PMID: 31159976
Cited by
-
Correlation between the vascular resistance index and arteriography for assessment of the distal arterial bed in chronic limb threatening ischemia.J Vasc Bras. 2024 Feb 5;23:e20230071. doi: 10.1590/1677-5449.202300712. eCollection 2024. J Vasc Bras. 2024. PMID: 38433983 Free PMC article.
References
-
- Ferraresi R, Palena LM, Mauri G, Manzi M. Tips and tricks for a correct “endo approach.”. J Cardiovasc Surg. 2013;54(6):685–711. - PubMed
-
- Palena LM. An extreme approach to CLI revascularization. Endovascular Today. 2016;15(5):68–72.
LinkOut - more resources
Full Text Sources