

Manipulative Reduction for Abnormal Uterine Inclination in Vaginal Delivery
- PMID: 35136417
- PMCID: PMC8818402
- DOI: 10.1155/2022/4765447
Manipulative Reduction for Abnormal Uterine Inclination in Vaginal Delivery
Abstract
Objective: To investigate the manipulative reduction in abnormal uterine inclination in vaginal delivery.
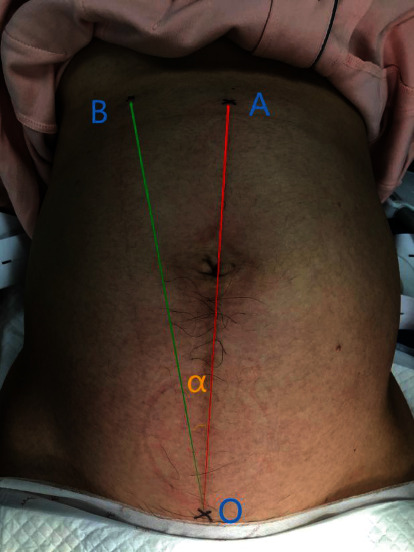
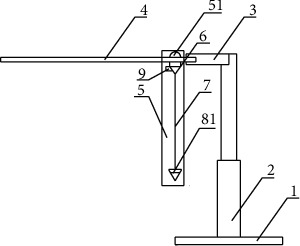
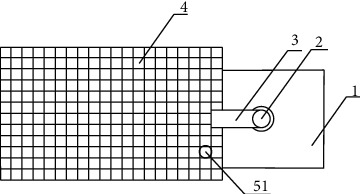
Methods: With the independently developed uterine inclination surveyor, 40 primiparas with abnormal uterine inclination were randomly divided into two groups: treatment group (Group A, 20 cases) and control group (Group B, 20 cases). The general condition of the primipara, the labor stages, the changes in uterine inclination after treatment, postpartum hemorrhage at 2 hours, and the general condition of fetuses were observed to study the therapeutic value of manual reduction in abnormal uterine inclination.
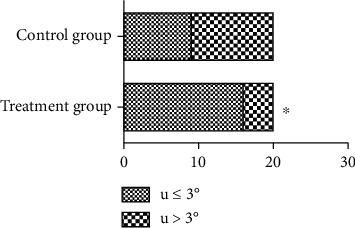
Result: In the control group, one uterine inclination was not corrected with the change in labor process, and the pregnancy was terminated due to stagnation of the active phase. In the first stage of labor, the time spent in the treatment group (393.4 ± 31.3 mins) was significantly lower than that in the control group (440.7 ± 34.9 mins) (P = 0.001). Compared with the control group (49.8 ± 6.5 mins), the treatment group (42.6 ± 7.2 mins) also exhibited a significantly shortened second stage of labor (P = 0.02). Sixteen cases (16/20) in the treatment group returned to normal after manual reduction, and 9 cases (9/20) in the control group returned to normal with the progression of natural labor. Manual reduction could be used as an option to treat abnormal uterine inclination (P = 0.01). There was no significant difference in the third stage of labor (P = 0.2), 2-hour postpartum hemorrhage (P = 0.35), Apgar score (P = 0.64), or body weight (P = 0.76) between the two groups.
Conclusion: Manual reduction in the treatment of abnormal uterine inclination has obvious effects, shortens the birth process, and is safe for the fetus.
Copyright © 2022 Jia Chen et al.
Conflict of interest statement
There is no conflict of interest.
Figures
Similar articles
-
[Effect of induced labor on delivery outcome of pregnant women undergoing vaginal trial of labor after cesarean section].Zhonghua Fu Chan Ke Za Zhi. 2019 Sep 25;54(9):582-587. doi: 10.3760/cma.j.issn.0529-567x.2019.09.002. Zhonghua Fu Chan Ke Za Zhi. 2019. PMID: 31550773 Chinese.
-
Complications of shoulder dystocia.Semin Perinatol. 2014 Jun;38(4):201-4. doi: 10.1053/j.semperi.2014.04.005. Semin Perinatol. 2014. PMID: 24863025 Review.
-
[Clinical study on vaginal birth after cesarean].Zhonghua Fu Chan Ke Za Zhi. 2016 Aug 25;51(8):586-91. doi: 10.3760/cma.j.issn.0529-567X.2016.08.007. Zhonghua Fu Chan Ke Za Zhi. 2016. PMID: 27561937 Clinical Trial. Chinese.
-
[Clinical study on perinatal outcomes of 80 cases with unicornuate uterus pregnancy].Zhonghua Fu Chan Ke Za Zhi. 2020 Aug 25;55(8):510-515. doi: 10.3760/cma.j.cn112141-20200107-00019. Zhonghua Fu Chan Ke Za Zhi. 2020. PMID: 32854474 Clinical Trial. Chinese.
-
Shoulder dystocia: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF).Eur J Obstet Gynecol Reprod Biol. 2016 Aug;203:156-61. doi: 10.1016/j.ejogrb.2016.05.047. Epub 2016 May 30. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 27318182 Review.
References
-
- Choi S. K., Park Y. G., Lee D. H., Ko H. S., Park I. Y., Shin J. C. Sonographic assessment of fetal occiput position during labor for the prediction of labor dystocia and perinatal outcomes. The Journal of Maternal-Fetal & Neonatal Medicine . 2016;29(24):3988–3992. doi: 10.3109/14767058.2016.1152250. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
