

Therapeutic strategies to remodel immunologically cold tumors
- PMID: 35136604
- PMCID: PMC8809427
- DOI: 10.1002/cti2.1226
Therapeutic strategies to remodel immunologically cold tumors
Abstract
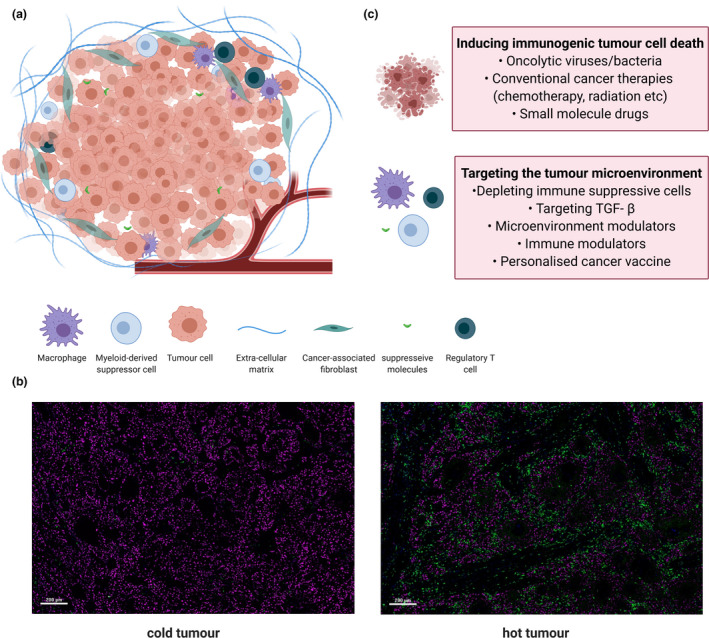
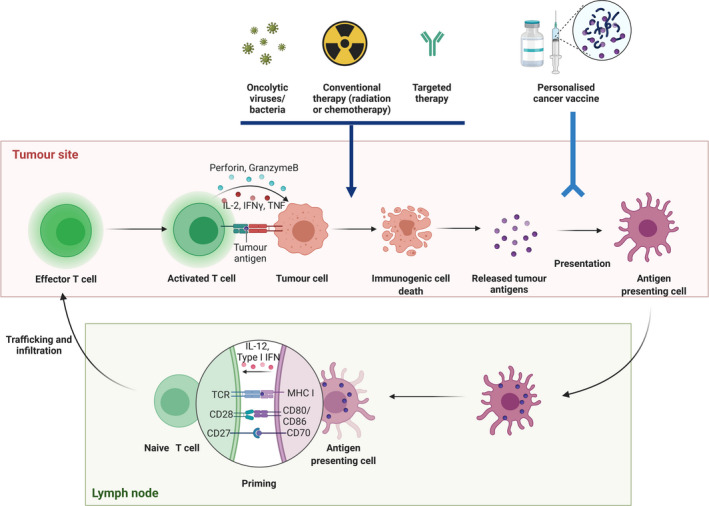
Immune checkpoint inhibitors (ICIs) induce a durable response in a wide range of tumor types, but only a minority of patients outside these 'responsive' tumor types respond, with some totally resistant. The primary predictor of intrinsic immune resistance to ICIs is the complete or near-complete absence of lymphocytes from the tumor, so-called immunologically cold tumors. Here, we propose two broad approaches to convert 'cold' tumors into 'hot' tumors. The first is to induce immunogenic tumor cell death, through the use of oncolytic viruses or bacteria, conventional cancer therapies (e.g. chemotherapy or radiation therapy) or small molecule drugs. The second approach is to target the tumor microenvironment, and covers diverse options such as depleting immune suppressive cells; inhibiting transforming growth factor-beta; remodelling the tumor vasculature or hypoxic environment; strengthening the infiltration and activation of antigen-presenting cells and/or effector T cells in the tumor microenvironment with immune modulators; and enhancing immunogenicity through personalised cancer vaccines. Strategies that successfully modify cold tumors to overcome their resistance to ICIs represent mechanistically driven approaches that will ultimately result in rational combination therapies to extend the clinical benefits of immunotherapy to a broader cancer cohort.
Keywords: cancer immunotherapy; cold tumor; immune checkpoint inhibitor; immune surveillance and resistance; therapeutic strategy; tumor microenvironment.
© 2020 The Authors. Clinical & Translational Immunology published by John Wiley & Sons Australia, Ltd on behalf of Australian and New Zealand Society for Immunology, Inc.
Conflict of interest statement
PJN received research grants from Roche/Genentech, BMS, Allergan, Compugen and Juno/Celgene, outside the submitted work. JD reports research support from Roche Genentech, Lilly, Astra Zeneca, BeiGene, Novartis, Bristol‐Myers Squibb and GlaxoSmithKline, and consulting fees from Amgen, Eisai and Pierre‐Fabre. The authors have no other conflicts of interest to declare.
Figures
References
-
- Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov 2019; 18: 197–218. - PubMed
Publication types
LinkOut - more resources
Full Text Sources