

Feasibility of arterial spin labeling in evaluating high- and low-flow peripheral vascular malformations: a case series
- PMID: 35136637
- PMCID: PMC8803223
- DOI: 10.1259/bjrcr.20210083
Feasibility of arterial spin labeling in evaluating high- and low-flow peripheral vascular malformations: a case series
Abstract
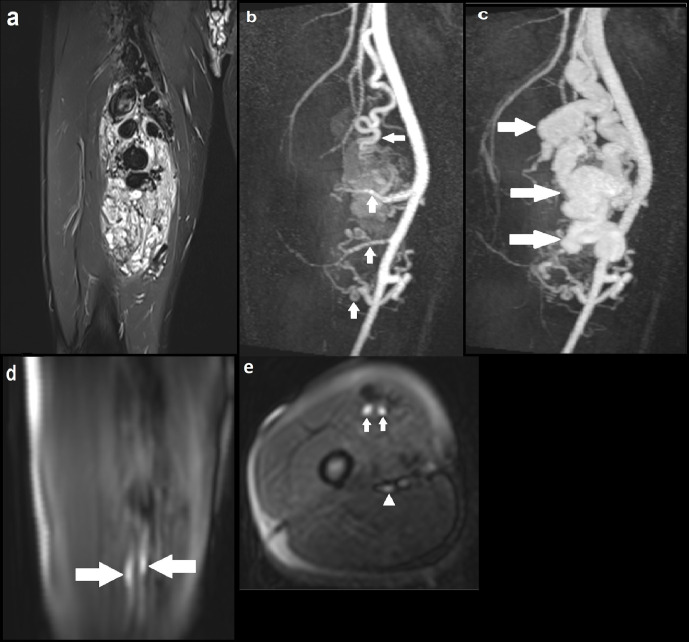
We present a case series highlighting a novel use of arterial spin labeling (ASL), a MRI perfusion technique, to evaluate both high- and low-flow peripheral vascular malformations (PVMs) across a range of anatomical locations. While the role of ASL in assessing intracranial vascular malformations is more established, there is limited evidence for PVMs. Our results provide preliminary evidence for the feasibility of ASL in imaging PVMs and its potential ability to distinguish between high- and low-flow PVMs. In addition, we demonstrate its ability to identify focal high blood flow, which may indicate the nidus in arteriovenous malformations. Together, these findings have important implications for patient management. We also outline the potential benefits and limitations of ASL in the imaging of PVMs, and provide justification for further validation of its diagnostic performance.
© 2022 The Authors. Published by the British Institute of Radiology.
Conflict of interest statement
Competing interests: The authors declare that they have no conflict of interest.
Figures





Similar articles
-
Novel use of arterial spin labelling in the imaging of peripheral vascular malformations.BJR Case Rep. 2020 Mar 24;6(3):20200021. doi: 10.1259/bjrcr.20200021. eCollection 2020 Sep 1. BJR Case Rep. 2020. PMID: 32922846 Free PMC article.
-
Arterial spin labeling magnetic resonance imaging: toward noninvasive diagnosis and follow-up of pediatric brain arteriovenous malformations.J Neurosurg Pediatr. 2015 Apr;15(4):451-8. doi: 10.3171/2014.9.PEDS14194. Epub 2015 Jan 30. J Neurosurg Pediatr. 2015. PMID: 25634818
-
Clinical and Arterial Spin Labeling Brain MRI Features of Transitional Venous Anomalies.J Neuroimaging. 2018 May;28(3):289-300. doi: 10.1111/jon.12487. Epub 2017 Dec 4. J Neuroimaging. 2018. PMID: 29205641
-
Mapping of cerebral perfusion territories using territorial arterial spin labeling: techniques and clinical application.NMR Biomed. 2013 Aug;26(8):901-12. doi: 10.1002/nbm.2836. Epub 2012 Jul 15. NMR Biomed. 2013. PMID: 22807022 Review.
-
A neuroradiologist's guide to arterial spin labeling MRI in clinical practice.Neuroradiology. 2015 Dec;57(12):1181-202. doi: 10.1007/s00234-015-1571-z. Epub 2015 Sep 9. Neuroradiology. 2015. PMID: 26351201 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
