

Anaphylaxis in Omani Patients: A Study from a Tertiary Care Center
- PMID: 35136659
- PMCID: PMC8804154
- DOI: 10.5001/omj.2021.113
Anaphylaxis in Omani Patients: A Study from a Tertiary Care Center
Abstract
Objectives: Anaphylaxis is an acute and potentially fatal allergic reaction. No studies have yet been conducted to evaluate the spectrum of anaphylactic reactions among Omani patients. As such, this study aimed to describe the clinical features, causes, investigation, and management of anaphylaxis among patients presenting to a tertiary care center in Oman.
Methods: This retrospective study took place between August 2005 and June 2020 at the allergy and immunology clinic of Sultan Qaboos University Hospital, Muscat, Oman. All patients diagnosed with anaphylaxis during the study period were included. Data were collected from electronic medical records.
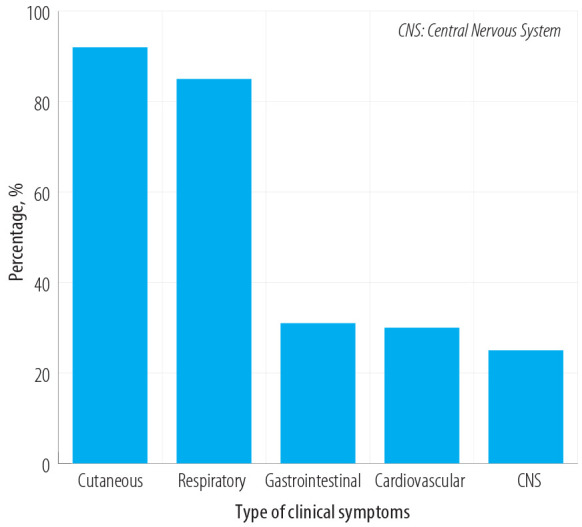
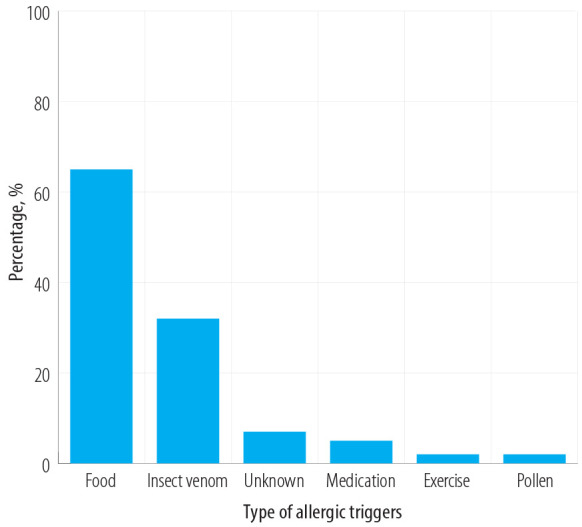
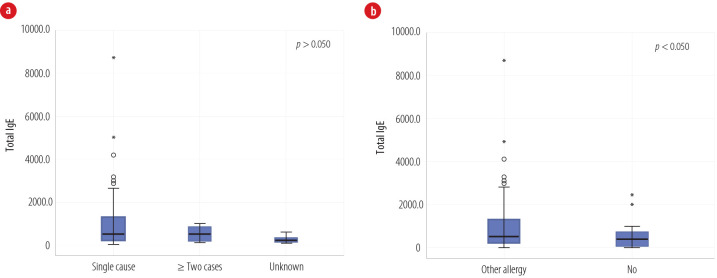
Results: One hundred patients were diagnosed with anaphylaxis during the study period. Of these, 52.0% were male. The mean age was 15.9±16.2 years, with 70.0% aged < 18 years old. The eosinophil count ranged from 0.0-16.9 × 109/L, with a mean of 0.8±2.2 × 109/L and a median of 0.3 (0.1-0.6) × 109/L. Total immunoglobulin (Ig) E levels ranged from 25-8706 kIU/L, with a mean of 935.1±1369.5 kIU/L and a median of 500.4 (186.0-972.5) kIU/L. The majority of patients had a family history of allergies (72.0%), and other had concomitant allergic conditions (66.0%). All were prescribed epinephrine (100%). The most common cause of anaphylaxis was food (65.0%). The second most frequent trigger was insect venom (32.0%). Most patients had one category cause (81.0%); two or more causes were present in 12.0% of patients. Clinical symptoms manifested most frequently as cutaneous (92.0%) and respiratory (85.0%). The majority of patients (87.0%) demonstrated the involvement of more than one bodily system. Mean total IgE levels were significantly higher in patients with concomitant presence of other allergic conditions (1193.8 kIU/L) than patients without another concomitant allergic disease (503.6 kIU/L; p =0.030). In addition, concomitant allergic disease is significantly higher in patients < 18 years of age (75.4%) compared to patients > 18 years of age (45.2%; p =0.010).
Conclusions: Due to its life-threatening nature, knowledge of the epidemiology and clinical features of anaphylaxis in different populations is necessary to deliver rapid treatment. This study found that the clinical features of anaphylactic patients in Oman were similar to those reported elsewhere. Further research is needed to determine the true incidence of anaphylaxis in Oman to minimize associated morbidity and mortality.
Keywords: Allergens; Anaphylaxis; Epinephrine; Immunoglobulin E; Retrospective Studies.
The OMJ is Published Bimonthly and Copyrighted 2022 by the OMSB.
Figures
Similar articles
-
Food Allergen Sensitisation Patterns in Omani Patients with Allergic Manifestations.Sultan Qaboos Univ Med J. 2018 Nov;18(4):e483-e488. doi: 10.18295/squmj.2018.18.04.009. Epub 2019 Mar 28. Sultan Qaboos Univ Med J. 2018. PMID: 30988967 Free PMC article.
-
Incidence of Optic Neuritis among Omani Patients with Multiple Sclerosis at the Sultan Qaboos University Hospital, Muscat, Oman.Sultan Qaboos Univ Med J. 2023 Nov;23(4):472-478. doi: 10.18295/squmj.5.2023.029. Epub 2023 Nov 30. Sultan Qaboos Univ Med J. 2023. PMID: 38090249 Free PMC article.
-
Anaphylaxis in a country where Asia and Europe meet: Evaluation according to World Allergy Organization (WAO) and European Academy of Allergy and Clinical Immunology (EAACI) diagnostic criteria.World Allergy Organ J. 2024 Sep 11;17(9):100962. doi: 10.1016/j.waojou.2024.100962. eCollection 2024 Sep. World Allergy Organ J. 2024. PMID: 39310371 Free PMC article.
-
Evaluation of red meat allergy patients and review of the literature.Turk J Pediatr. 2021;63(5):832-845. doi: 10.24953/turkjped.2021.05.011. Turk J Pediatr. 2021. PMID: 34738365 Review.
-
Anaphylaxis in Children and Adolescents.Immunol Allergy Clin North Am. 2021 Nov;41(4):627-638. doi: 10.1016/j.iac.2021.07.009. Immunol Allergy Clin North Am. 2021. PMID: 34602233 Review.
Cited by
-
Anaphylactic reaction as an etiology of ischemic stroke: A case report.Radiol Case Rep. 2023 Sep 26;18(12):4313-4317. doi: 10.1016/j.radcr.2023.08.110. eCollection 2023 Dec. Radiol Case Rep. 2023. PMID: 37789922 Free PMC article.
-
Prevalence of immunoglobulin E sensitization to various inhaled allergens among the residents of the Northern United Arab Emirates: Automated evaluation of a membrane-based test system.Saudi Med J. 2025 Mar;46(3):282-291. doi: 10.15537/smj.2025.46.3.20240929. Saudi Med J. 2025. PMID: 40096981 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials