

Approach to the Patient With Lipodystrophy
- PMID: 35137140
- PMCID: PMC9113814
- DOI: 10.1210/clinem/dgac079
Approach to the Patient With Lipodystrophy
Abstract
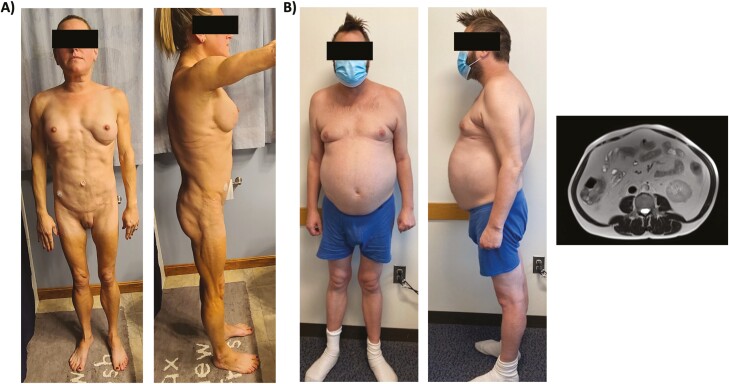
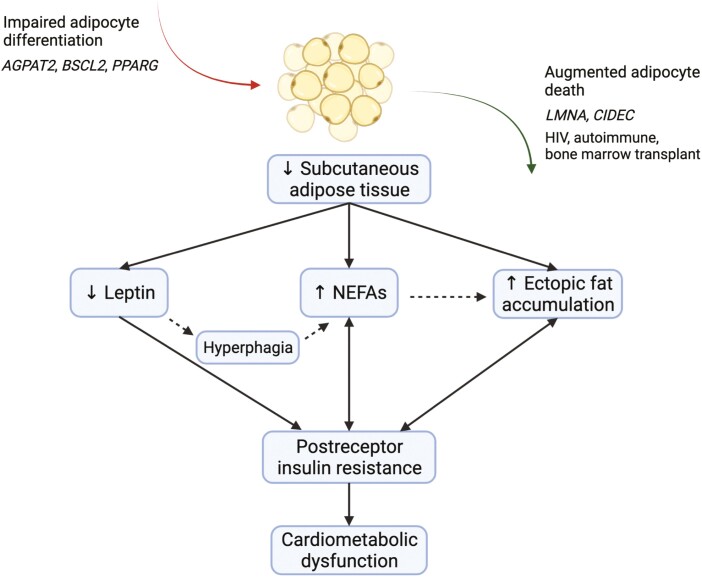
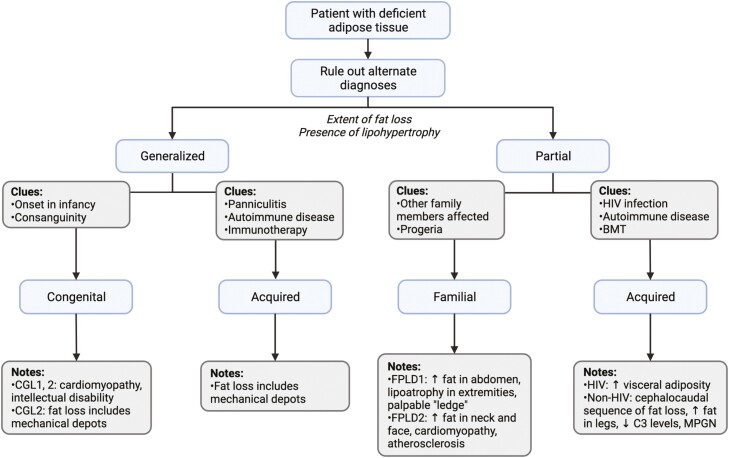
Lipodystrophy constitutes a spectrum of diseases characterized by a generalized or partial absence of adipose tissue. Underscoring the role of healthy fat in maintenance of metabolic homeostasis, fat deficiency in lipodystrophy typically leads to profound metabolic disturbances including insulin resistance, hypertriglyceridemia, and ectopic fat accumulation. While rare, recent genetic studies indicate that lipodystrophy is more prevalent than has been previously thought, suggesting considerable underdiagnosis in clinical practice. In this article, we provide an overview of the etiology and management of generalized and partial lipodystrophy disorders. We bring together the latest scientific evidence and clinical guidelines and expose key gaps in knowledge. Through improved recognition of the lipodystrophy disorders, patients (and their affected family members) can be appropriately screened for cardiometabolic, noncardiometabolic, and syndromic abnormalities and undergo treatment with targeted interventions. Notably, insights gained through the study of this rare and extreme phenotype can inform our knowledge of more common disorders of adipose tissue overload, including generalized obesity.
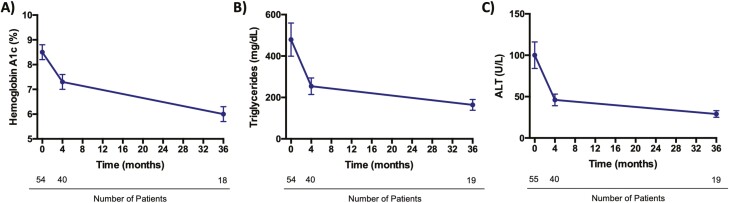
Keywords: Dunnigan variety lipodystrophy; HIV-associated lipodystrophy; lipodystrophy; metreleptin; tesamorelin.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Agarwal AK, Garg A. Genetic disorders of adipose tissue development, differentiation, and death. Annu Rev Genomics Hum Genet. 2006;7:175-199. - PubMed
-
- Gonzaga-Jauregui C, Ge W, Staples J, et al. . Clinical and molecular prevalence of lipodystrophy in an unascertained large clinical care cohort. Diabetes. 2020;69(2):249-258. - PubMed
-
- Frayn KN. Adipose tissue as a buffer for daily lipid flux. Diabetologia. 2002;45(9):1201-1210. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
