

Effect of laparoscopic sleeve gastrectomy vs laparoscopic sleeve + Rossetti fundoplication on weight loss and de novo GERD in patients affected by morbid obesity: a randomized clinical study
- PMID: 35137287
- PMCID: PMC9055016
- DOI: 10.1007/s11695-022-05955-8
Effect of laparoscopic sleeve gastrectomy vs laparoscopic sleeve + Rossetti fundoplication on weight loss and de novo GERD in patients affected by morbid obesity: a randomized clinical study
Erratum in
-
Correction to: Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Sleeve + Rossetti Fundoplication on Weight Loss and De Novo GERD in Patients Affected by Morbid Obesity: a Randomized Clinical Study.Obes Surg. 2022 Jun;32(6):2102. doi: 10.1007/s11695-022-06013-z. Obes Surg. 2022. PMID: 35325449 Free PMC article. No abstract available.
Abstract
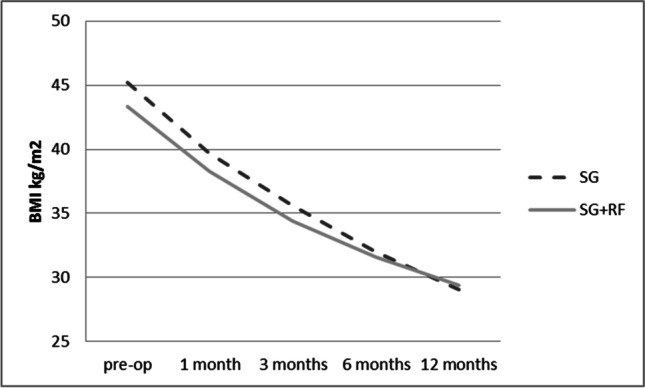
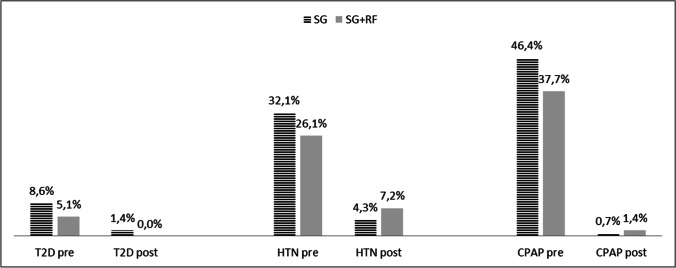
Purpose: To compare sleeve gastrectomy (SG) to SG associated with Rossetti fundoplication (SG + RF) in terms of de novo gastro-esophageal reflux disease (GERD) after surgery, weight loss, and postoperative complications.
Materials and methods: Patients affected by morbid obesity, without symptoms of GERD, who were never in therapy with proton pump inhibitors (PPIs), were randomized into two groups. One group underwent SG and the other SG + RF. The study was stopped on February 2020 due to the COVID pandemic.
Results: A total of 278 patients of the programmed number of 404 patients were enrolled (68.8%). De novo esophagitis was considered in those patients who had both pre- and postoperative gastroscopy (97/278, 34.9%). Two hundred fifty-one patients (90.3%) had completed clinical follow-up at 12 months. SG + RF resulted in an adequate weight loss, similar to classic SG at 12-month follow-up (%TWL = 35. 4 ± 7.2%) with a significantly better outcome in terms of GERD development. One year after surgery, PPIs were necessary in 4.3% SG + RF patients compared to 17.1% SG patients (p = 0.001). Esophagitis was present in 2.0% of SG + RF patients versus 23.4% SG patients (p = 0.002). The main complication after SG + RF was wrap perforation (4.3%), which improved with the surgeon's learning curve.
Conclusion: SG + RF seemed to be an effective alternative to classic SG in preventing de novo GERD. More studies are needed to establish that an adequate learning curve decreases the higher percentage of short-term complications in the SG + RF group.
Keywords: GERD; Nissen sleeve; Obesity; Rossetti sleeve.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
All the authors declare no competing interests.
Figures
References
-
- Sharma A, Aggarwal S, Ahuja V, Bal C. Evaluation of gastroesophageal reflux before and after sleeve gastrectomy using symptom scoring, scintigraphy, and endoscopy. Surg Obes Relat Dis. 2014 Jul-Aug;10(4):600–5. 10.1016/j.soard.2014.01.017. Epub 2014 Jan 28. PMID: 24837563. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
