

Cost-Effectiveness of Dapagliflozin for Non-diabetic Chronic Kidney Disease
- PMID: 35137296
- PMCID: PMC9551016
- DOI: 10.1007/s11606-021-07311-5
Cost-Effectiveness of Dapagliflozin for Non-diabetic Chronic Kidney Disease
Abstract
Background: In the USA, chronic kidney disease (CKD) affects 1 in 7 adults and costs $100 billion annually. The DAPA-CKD trial found dapagliflozin, a sodium glucose co-transporter 2 (SGLT2) inhibitor, to be effective in reducing CKD progression and mortality in patients with diabetic and non-diabetic CKD. Currently, SGLT2 inhibitors are not considered standard of care for patients with non-diabetic CKD.
Objective: Determine the cost-effectiveness of adding dapagliflozin to standard management of patients with non-diabetic CKD.
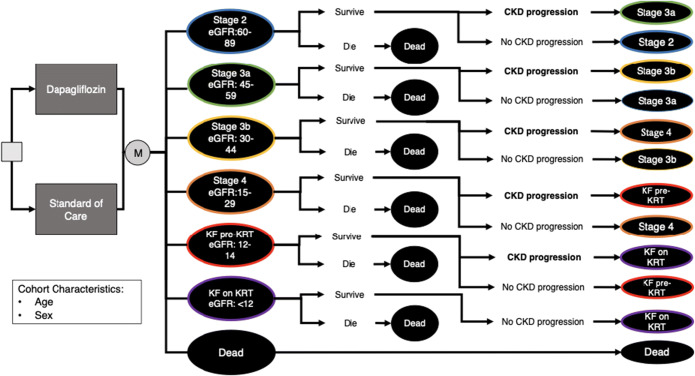
Design: Markov model with lifetime time horizon and US healthcare sector perspective.
Patients: Patients with non-diabetic CKD INTERVENTION: Dapagliflozin plus standard care versus standard care only.
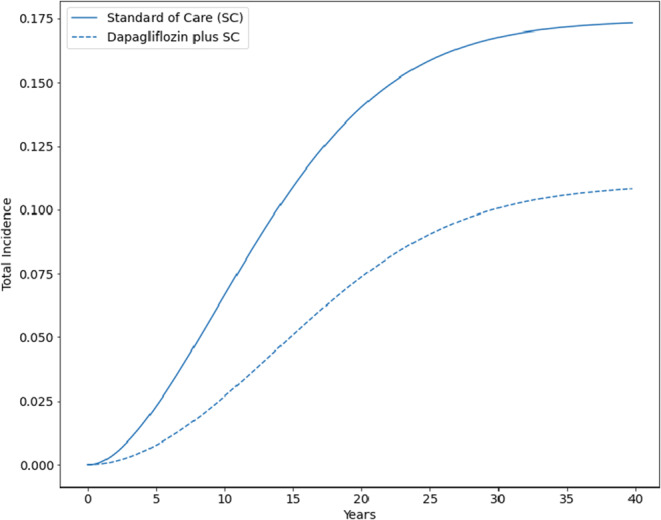
Main measures: Quality-adjusted life years (QALYs), costs, and incremental cost-effectiveness ratios (ICERs), all discounted at 3% annually; total incidence of kidney failure on kidney replacement therapy; average years on kidney replacement therapy.
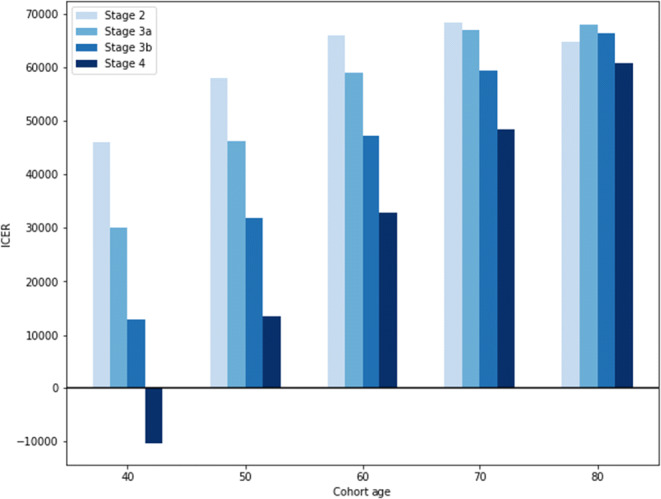
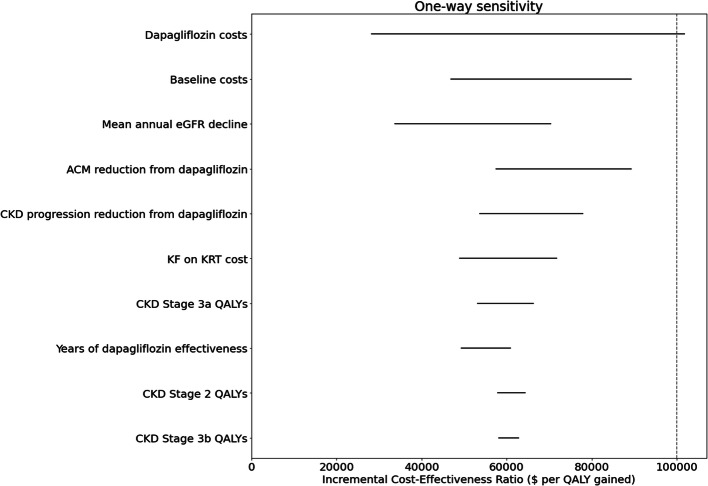
Key results: Adding dapagliflozin to standard care improved life expectancy by 2 years, increased discounted QALYS (from 6.75 to 8.06), and reduced the total incidence of kidney failure on kidney replacement therapy (KRT) (from 17.4 to 11.0%) and average years on KRT (from 0.77 to 0.43) over the lifetime of the cohort. Dapagliflozin plus standard care was more effective than standard care alone while increasing lifetime costs (from $245,900 to $324,8900, or $60,000 per QALY gained). Results were robust to variations in assumptions about dapagliflozin's efficacy over time and by CKD stage, added costs of kidney replacement therapy, and expected population annual CKD progression rates and sensitive to the cost of dapagliflozin. The net 1-year budgetary implication of treating all US patients with non-diabetic CKD could be up to $21 billion.
Conclusions: Dapagliflozin improved life expectancy and reduced progression of CKD, the proportion of patients requiring kidney replacement therapy, and time on kidney replacement therapy in patients with non-diabetic CKD. Use of dapagliflozin meets conventional criteria for cost-effectiveness.
Keywords: chronic kidney disease; cost-effectiveness analysis; health economics.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
Dr. Chertow served on the Steering Committee of the DAPA-CKD trial. All other authors have nothing to disclose.
Figures
References
-
- Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data [Internet]. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2019. Accessed 30 Dec 2021 from: https://www.cdc.gov/nchs/nhanes/index.htm
-
- United States Renal Data System. 2019 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
