

Early post-discharge mortality in CAP: frequency, risk factors and a prediction tool
- PMID: 35137301
- PMCID: PMC8934328
- DOI: 10.1007/s10096-022-04416-5
Early post-discharge mortality in CAP: frequency, risk factors and a prediction tool
Abstract
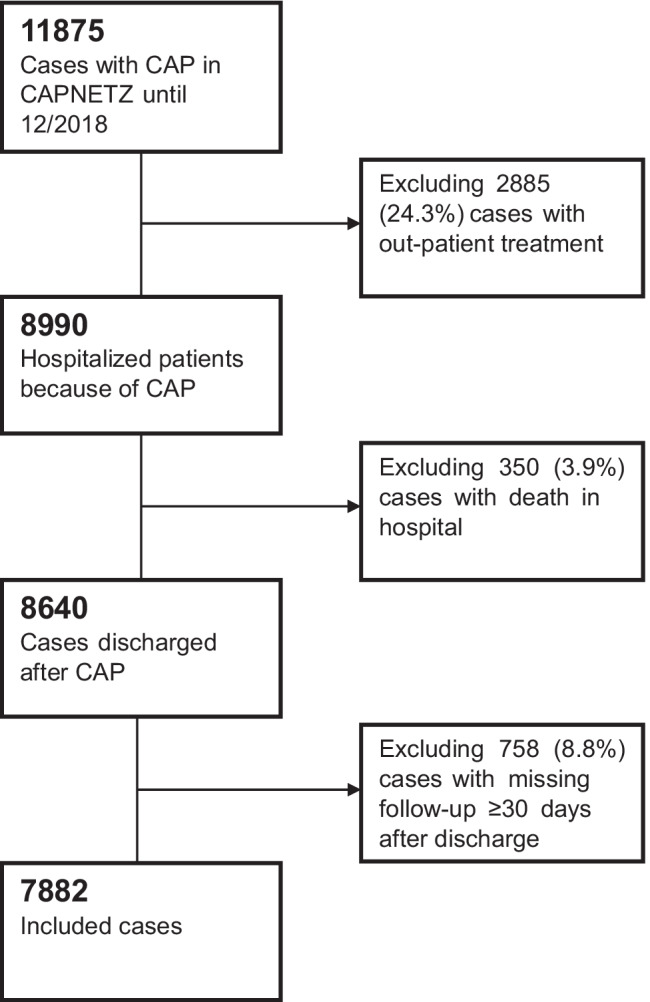
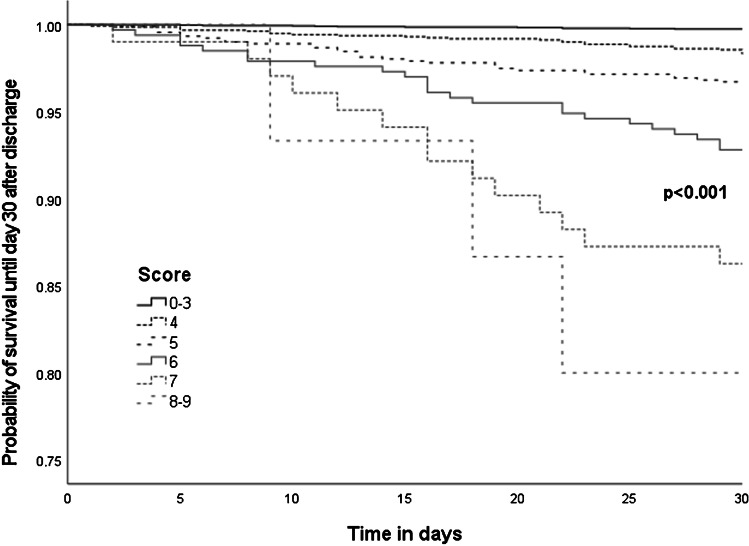
There are few data on mortality after discharge with community-acquired pneumonia (CAP). Therefore, we evaluated risk factors for 30-day post-discharge mortality after CAP. We included all patients of the prospective multi-national CAPNETZ study between 2002 and 2018 with (1) hospitalized CAP, (2) survival until discharge, and (3) complete follow-up data. The study endpoint was death within 30 days after discharge. We evaluated risk factors including demographics, comorbidities, admission CAP severity, and laboratory values and treatment-related factors in uni- and multivariable analyses. A total of 126 (1.6%) of 7882 included patients died until day 30 after discharge, corresponding to 26% of all 476 deaths. After multivariable analysis, we identified 10 independent risk factors: higher age, lower BMI, presence of diabetes mellitus, chronic renal or chronic neurological disease (other than cerebrovascular diseases), low body temperature or higher thrombocytes on admission, extended length of hospitalization, oxygen therapy during hospitalization, and post-obstructive pneumonia. By addition these factors, we calculated a risk score with an AUC of 0.831 (95%CI 0.822-0.839, p < 0.001) for prediction of post-discharge mortality. Early post-discharge deaths account for ¼ of all CAP-associated deaths and are associated with patient- and CAP-severity-related risk factors. Additional studies are necessary to replicate our findings in independent cohorts. Study registration: NCT02139163.
Keywords: Community-acquired pneumonia; Mortality; Post-discharge; Prognosis.
© 2022. The Author(s).
Conflict of interest statement
Dr. Pletz reports grants from Pfizer and consulting fees or honoraria for lectures or advisory boards from Pfizer, MSD, Brahms, Novartis, and Chiesi, all outside the submitted work.
Dr. Rohde reports consulting fees or honoraria for lectures or advisory boards from Astra Zeneca, Berlin Chemie, BMS, Boehringer Ingelheim, Chiesi, Essex Pharma, Grifols, GSK, Insmed, MSD, Roche, Solvay, Takeda, Novartis, Pfizer, and Vertex, all outside the submitted work.
Dr. Kolditz reports grants from Pfizer and consulting fees or honoraria for lectures or advisory boards from BerlinChemie, Böhringer, MSD, AstraZeneca, Biotest, Novartis, Pfizer, GSK, Gilead, and Sanofi, all outside the submitted work.
Dr. Witzenrath reports grants from Deutsche Forschungsgemeinschaft, Bundesministerium für Bildung und Forschung, Marie Curie Foundation, Capnetz Stiftung, Noxxon, Pantherna, Vaxxilon, Bayer Health Care, Biotest; and consulting fees or honoraria from Noxxon, Pantherna, Silence Therapeutics, Vaxxilon, Aptarion, Glaxo Smith Kline, Sinoxa, Biotest, Astra Zeneca, Berlin Chemie, Chiesi, Novartis, Teva, Actelion, Boehringer Ingelheim, and Bayer Health Care, all outside the submitted work.
Ms. Glöckner and Barten-Neiner declare no conflict of interests relevant to the content of the article.
Figures
References
-
- Holter JC, Ueland T, Jenum PA, Muller F, Brunborg C, Froland SS, Aukrust P, Husebye E, Heggelund L. Risk factors for long-term mortality after hospitalization for community-acquired pneumonia: a 5-year prospective follow-up study. PLoS One. 2016;11(2):e0148741. doi: 10.1371/journal.pone.0148741. - DOI - PMC - PubMed
-
- Bruns AH, Oosterheert JJ, Cucciolillo MC, El MR, Groenwold RH, Prins JM, Hoepelman AI. Cause-specific long-term mortality rates in patients recovered from community-acquired pneumonia as compared with the general Dutch population. Clin Microbiol Infect. 2011;17(5):763–768. doi: 10.1111/j.1469-0691.2010.03296.x. - DOI - PubMed
-
- Wadhera RK, Joynt Maddox KE, Wasfy JH, Haneuse S, Shen C, Yeh RW. Association of the hospital readmissions reduction program with mortality among medicare beneficiaries hospitalized for heart failure, acute myocardial infarction, and pneumonia. JAMA. 2018;320(24):2542–2552. doi: 10.1001/jama.2018.19232. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
